

This is a preprint.
A spatially mapped gene expression signature for intestinal stem-like cells identifies high-risk precursors of gastric cancer
- PMID: 37786704
- PMCID: PMC10541579
- DOI: 10.1101/2023.09.20.558462
A spatially mapped gene expression signature for intestinal stem-like cells identifies high-risk precursors of gastric cancer
Update in
-
A spatial transcriptomic signature of 26 genes resolved at single-cell resolution characterizes high-risk gastric cancer precursors.NPJ Precis Oncol. 2025 Feb 25;9(1):52. doi: 10.1038/s41698-025-00816-w. NPJ Precis Oncol. 2025. PMID: 40000871 Free PMC article.
Abstract
Objective: Gastric intestinal metaplasia (GIM) is a precancerous lesion that increases gastric cancer (GC) risk. The Operative Link on GIM (OLGIM) is a combined clinical-histopathologic system to risk-stratify patients with GIM. The identification of molecular biomarkers that are indicators for advanced OLGIM lesions may improve cancer prevention efforts.
Methods: This study was based on clinical and genomic data from four cohorts: 1) GAPS, a GIM cohort with detailed OLGIM severity scoring (N=303 samples); 2) the Cancer Genome Atlas (N=198); 3) a collation of in-house and publicly available scRNA-seq data (N=40), and 4) a spatial validation cohort (N=5) consisting of annotated histology slides of patients with either GC or advanced GIM. We used a multi-omics pipeline to identify, validate and sequentially parse a highly-refined signature of 26 genes which characterize high-risk GIM.
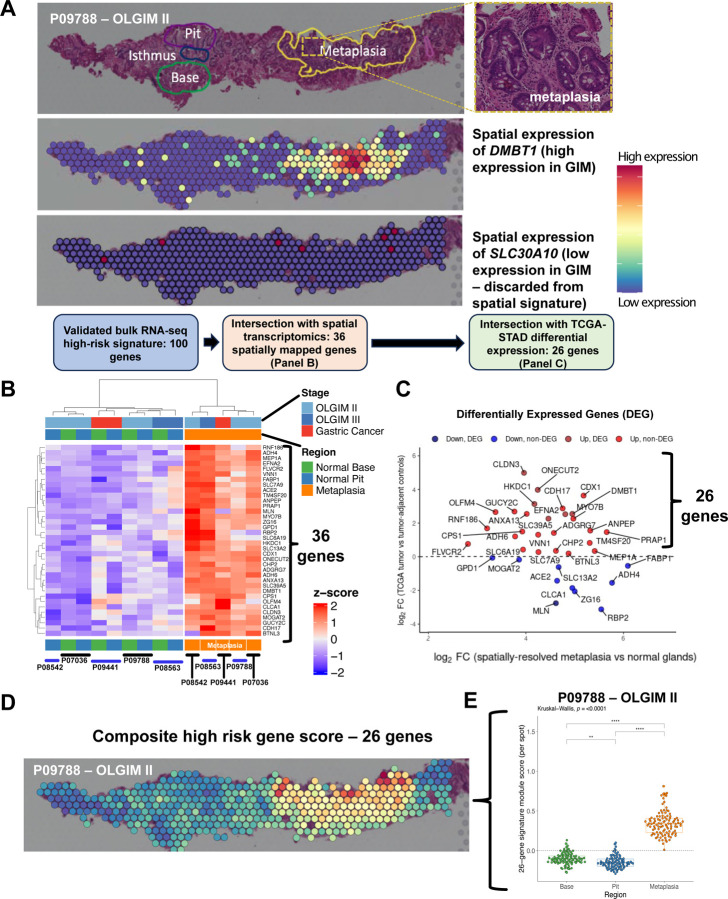
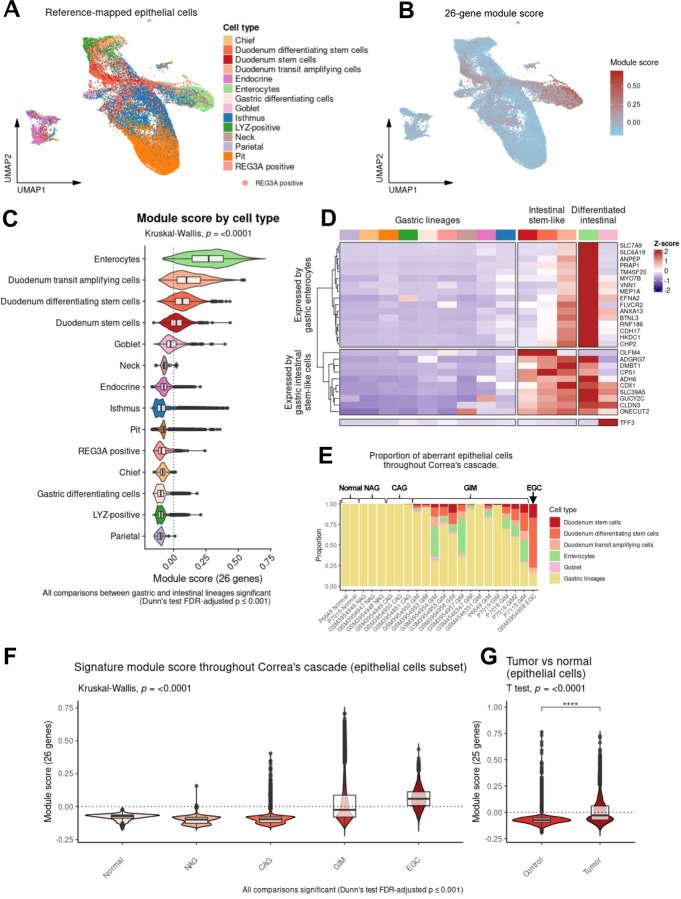
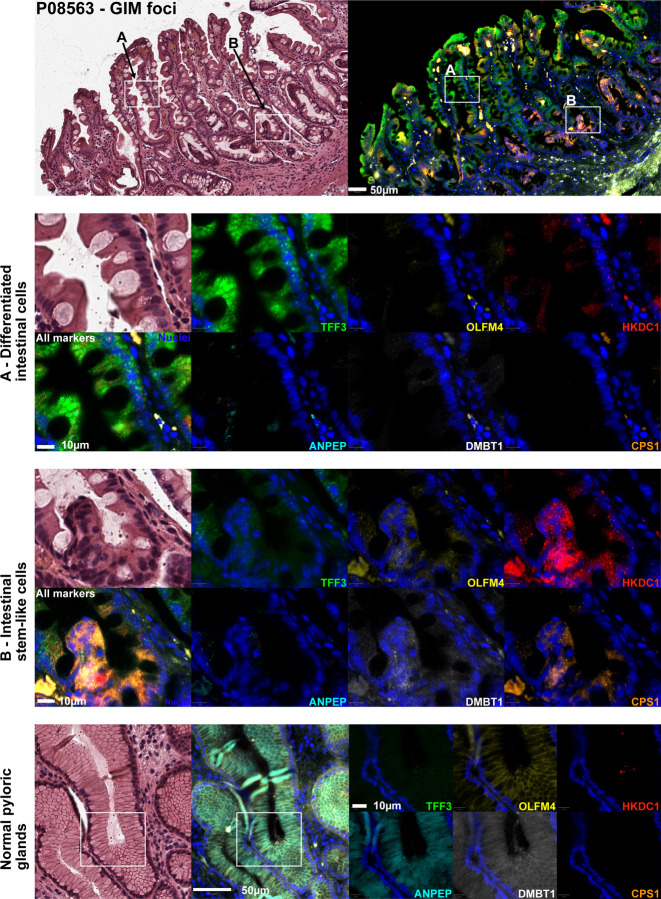
Results: Using standard RNA-seq, we analyzed two separate, non-overlapping discovery (N=88) and validation (N=215) sets of GIM. In the discovery phase, we identified 105 upregulated genes specific for high-risk GIM (defined as OLGIM III-IV), of which 100 genes were independently confirmed in the validation set. Spatial transcriptomic profiling revealed 36 of these 100 genes to be expressed in metaplastic foci in GIM. Comparison with bulk GC sequencing data revealed 26 of these genes to be expressed in intestinal-type GC. Single-cell profiling resolved the 26-gene signature to both mature intestinal lineages (goblet cells, enterocytes) and immature intestinal lineages (stem-like cells). A subset of these genes was further validated using single-molecule multiplex fluorescence in situ hybridization. We found certain genes (TFF3 and ANPEP) to mark differentiated intestinal lineages, whereas others (OLFM4 and CPS1) localized to immature cells in the isthmic/crypt region of metaplastic glands, consistent with the findings from scRNAseq analysis.
Conclusions: using an integrated multi-omics approach, we identified a novel 26-gene expression signature for high-OLGIM precursors at increased risk for GC. We found this signature localizes to aberrant intestinal stem-like cells within the metaplastic microenvironment. These findings hold important translational significance for future prevention and early detection efforts.
Keywords: Intestinal metaplasia; OLGIM; gastric cancer; stem cells.
Conflict of interest statement
Competing interests The authors declare that they have no competing interests.
Figures


References
-
- Sung H. et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 71, 209–249 (2021). https://doi.org: 10.3322/caac.21660 - DOI - PubMed
-
- Allemani C. et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 391, 1023–1075 (2018). https://doi.org: 10.1016/S0140-6736(17)33326-3 - DOI - PMC - PubMed
-
- Correa P. Human gastric carcinogenesis: a multistep and multifactorial process--First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention. Cancer Res 52, 6735–6740 (1992). - PubMed
-
- Hwang Y. J. et al. Reversibility of atrophic gastritis and intestinal metaplasia after Helicobacter pylori eradication - a prospective study for up to 10 years. Aliment Pharmacol Ther 47, 380–390 (2018). https://doi.org: 10.1111/apt.14424 - DOI - PubMed
-
- Ito M. et al. Clinical prevention of gastric cancer by Helicobacter pylori eradication therapy: a systematic review. J Gastroenterol 44, 365–371 (2009). https://doi.org: 10.1007/s00535-009-0036-8 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous