

Evidence on Buprenorphine Dose Limits: A Review
- PMID: 37788601
- PMCID: PMC10547105
- DOI: 10.1097/ADM.0000000000001189
Evidence on Buprenorphine Dose Limits: A Review
Abstract
Objectives: As overdose deaths from fentanyl continue to increase, optimizing use of medications for opioid use disorder has become increasingly important. Buprenorphine is a highly effective medication for reducing the risk of overdose death, but only if a patient remains in treatment. Shared decision making between prescribers and patients is important to establish a dose that meets each patient's treatment needs. However, patients frequently face a dose limit of 16 or 24 mg/d based on dosing guidelines on the Food and Drug Administration's package label.
Methods: This review discusses patient-centered goals and clinical criteria for determining dose adequacy, reviews the history of buprenorphine dose regulation in the United States, examines pharmacological and clinical research results with buprenorphine doses up to 32 mg/d, and evaluates whether diversion concerns justify maintaining a low buprenorphine dose limit.
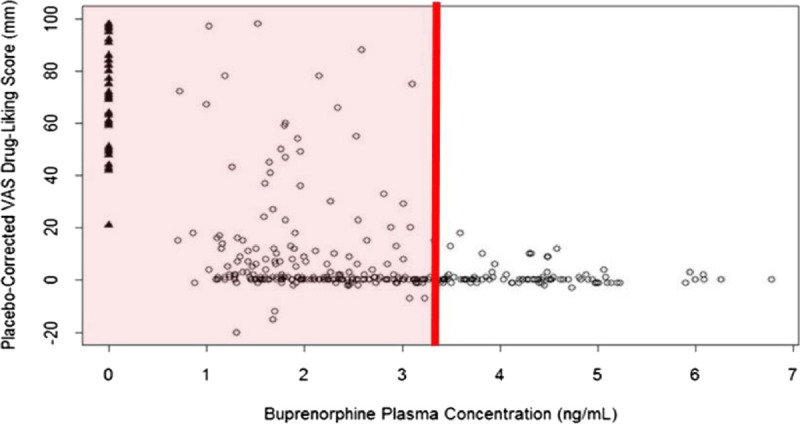
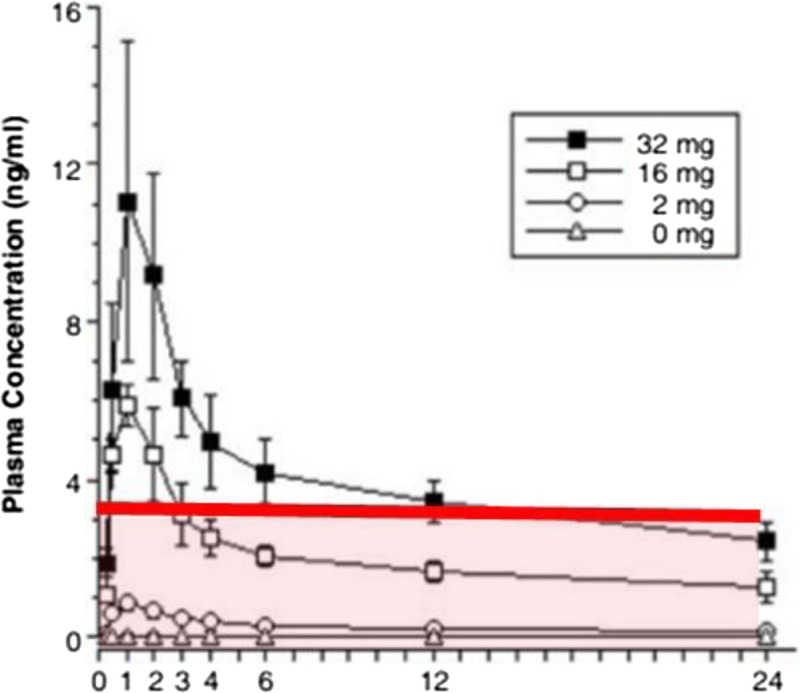
Results: Pharmacological and clinical research results consistently demonstrate buprenorphine's dose-dependent benefits up to at least 32 mg/d, including reductions in withdrawal symptoms, craving, opioid reward, and illicit use while improving retention in care. Diverted buprenorphine is most often used to treat withdrawal symptoms and reduce illicit opioid use when legal access to it is limited.
Conclusions: In light of established research and profound harms from fentanyl, the Food and Drug Administration's current recommendations on target dose and dose limit are outdated and causing harm. An update to the buprenorphine package label with recommended dosing up to 32 mg/d and elimination of the 16 mg/d target dose would improve treatment effectiveness and save lives.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Society of Addiction Medicine.
Figures
References
-
- Ahmad FB, Rossen LM, Sutton P. Provisional Drug Overdose Death Counts. Hyattsville, MD: National Center for Health Statistics, 2022. Available at: https://www.cdc.gov/nchs/nvss/vsrr/drug-overdose-data.htm. Accessed May 8, 2022.
-
- Volpe DA McMahon Tobin GA Mellon RD, et al. . Uniform assessment and ranking of opioid μ receptor binding constants for selected opioid drugs. Regul Toxicol Pharmacol. 2011;59(3):385–390. - PubMed
-
- Substance Abuse and Mental Health Services Administration . TIP 63: Medications for opioid use disorders—Full document. 2021. Available at: https://store.samhsa.gov/product/TIP-63-Medications-for-Opioid-Use-Disor.... Accessed August 4, 2022. - PubMed
-
- Wakeman SE Chang Y Regan S, et al. . Impact of fentanyl use on buprenorphine treatment retention and opioid abstinence. J Addict Med. 2019;13(4):253–257. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
