

Clinical long-term outcome of hepatitis D compared to hepatitis B monoinfection
- PMID: 37789170
- PMCID: PMC10661878
- DOI: 10.1007/s12072-023-10575-0
Clinical long-term outcome of hepatitis D compared to hepatitis B monoinfection
Abstract
Background and aims: Hepatitis D virus (HDV) infection causes the most severe form of chronic viral hepatitis. However, it is still unclear to what extent the underlying cirrhosis may contribute to disease progression. The aim of this study was to compare the long-term outcome of HDV infection with HBV monoinfection in a single-center cohort of both non-cirrhotic and cirrhotic patients.
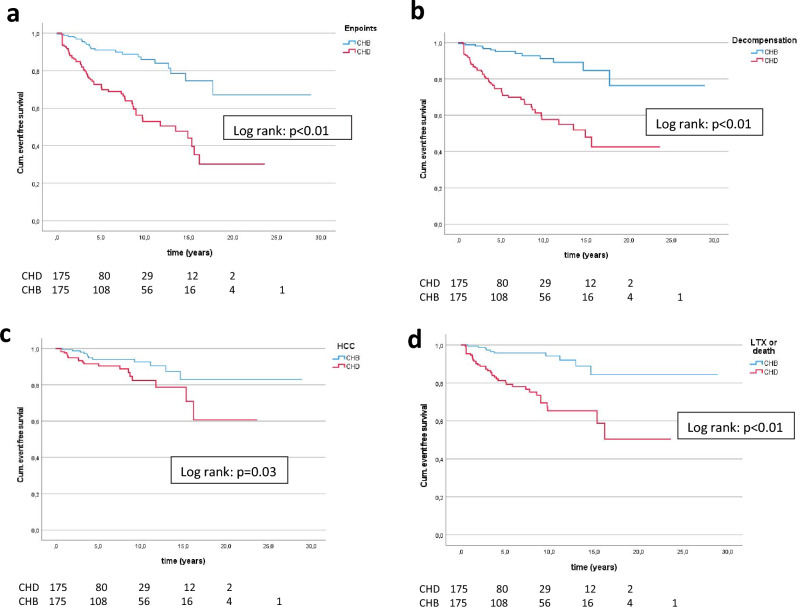
Method: We retrospectively studied 175 patients with chronic hepatitis D (CHD) who were followed for at least 6 months (median of 6.3 (0.6-23.6) years). In addition, we selected 175 patients with HBV monoinfection (CHB) who were matched for gender, age, region of origin, HBeAg status, and bilirubin. Liver-related clinical end points were defined as hepatic decompensation (ascites, encephalopathy, variceal bleeding), liver transplantation, HCC, or liver-related death.
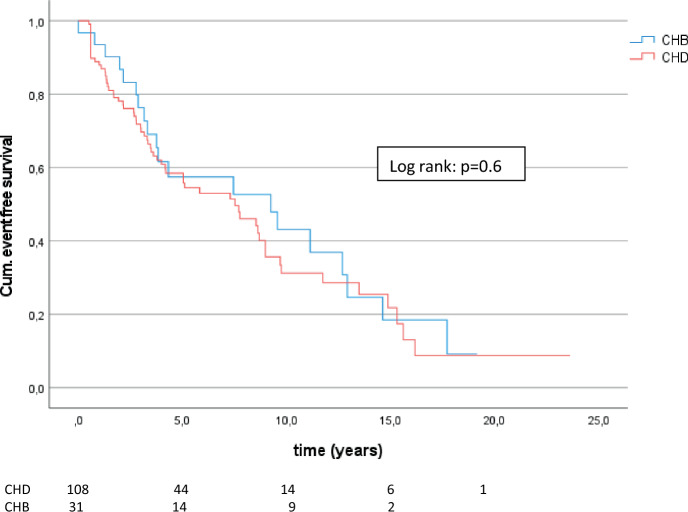
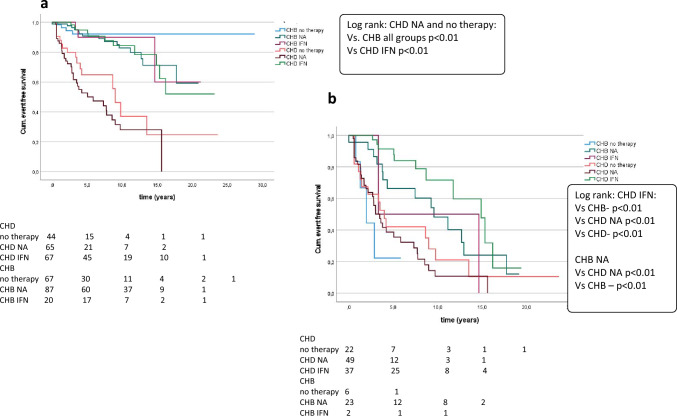
Results: Clinical complications developed earlier (4.6 vs. 6.2 years) and more frequently (35.4% vs. 12.6%, p < 0.01) in CHD patients. In a multivariate Cox regression, HDV infection was independently associated with the development of end points (p < 0.01; HR: 3.0; 95% CI 1.4-6.4). However, in cirrhotic patients there were no significant differences between HBV and HDV in the development of end points. Besides, CHB patients with cirrhosis developed more frequently HCC (35.5%) than CHD patients with cirrhosis (18.5%).
Conclusion: Our results confirmed that HDV leads to a faster progression to cirrhosis compared to HBV. However, once cirrhosis is present, not HDV but the underlying cirrhosis is the dominate intrinsic risk factor for the development of liver-related end points and for the progression to HCC.
Keywords: Cirrhosis; Clinical longterm outcome; HBeAg; Hepatitis B; Hepatitis delta; Hepatocellular carcinoma; Liver decompensation; Nucleos(t)ide analogs; Pegylated interferon alpha; Therapy.
© 2023. The Author(s).
Conflict of interest statement
Anika Wranke, Benjamin Heidrich, Katharina Luise Hupa-Breier, Janina Kirschner, and Birgit Bremer declare that they have no conflict of interest. Heiner Wedemeyer serves as clinical trials principal investigator for Abbvie, Altimmune, BMS, Gilead, Janssen, Merck/MSD, MYR GmbH, Novartis, and Vir Biotechnology, has research grants from Abbvie, Biotest, Gilead, Merck/MSD, and Roche, and advises or is on the speakers’ bureau for AbbVie, Aligos, Altimmune, Biotest, BMS, BTG, Dicerna, Enanta, Gilead, Janssen, Merck/MSD, MYR GmbH, Roche, and Vir Biotechnology. Markus Cornberg received honoraria for lectures or consulting from AbbVie, AiCuris, Falk, Gilead, GlaxoSmithKline (GSK), Janssen, Merck/MSD, Novartis, Roche, Swedish Orphan Biovitrum (SOBI). Katja Deterding received lecture fees and is on the advisory board for Gilead.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
