

A Case of Acute Extensive Viral Sinusitis Secondary to Acute Epstein Barr Virus
- PMID: 37789985
- PMCID: PMC10545147
- DOI: 10.12890/2023_004039
A Case of Acute Extensive Viral Sinusitis Secondary to Acute Epstein Barr Virus
Abstract
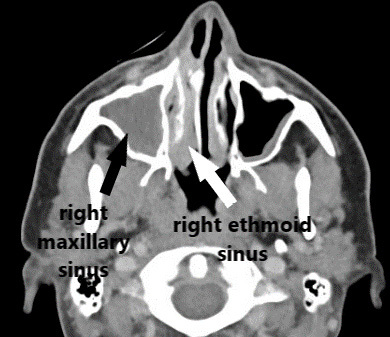
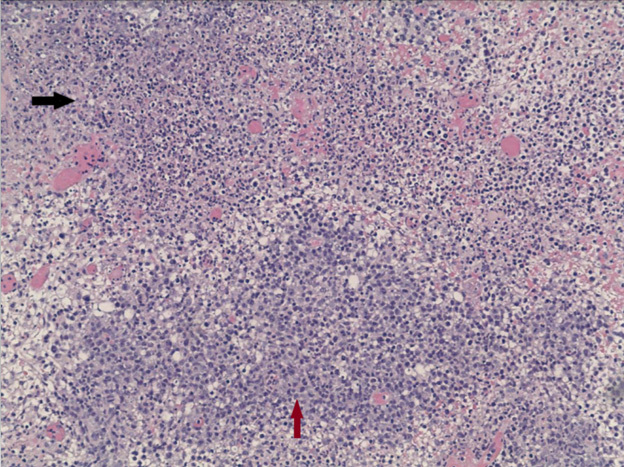
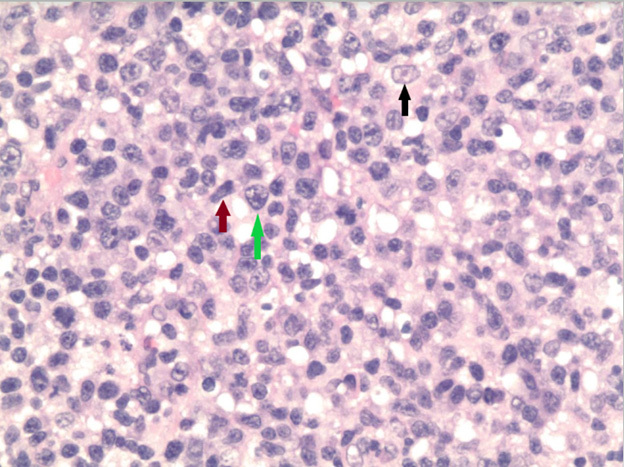
Infectious mononucleosis (IM), the most common presentation of acute Epstein Barr virus (EBV) infection, typically presents with fever, pharyngitis and lymphadenopathy. We describe an unusual case of IM presenting as acute sinusitis. A 25 year-old male presented to the emergency department with worsening right frontal sinus pain along with fever, chills, and greenish nasal discharge for 3 weeks. Laboratory workup showed leukocytosis with high lymphocyte counts as well as transaminitis. Facial computerized tomography (CT) showed extensive right frontal, ethmoidal and maxillary sinusitis and antrochoanal polyp. The patient underwent endoscopy with drainage of purulent material and polyp removal. Unfortunately, cultures of the sample were not sent and bacterial infection could not be ruled out. Broad spectrum antibiotics were continued. Pathology of redundant tissue revealed large atypical lymphocytes with positive EBV-encoded RNA and lack of evidence of extranodal natural killer/T-cell (NK/T-cell) type lymphoma (ENKTCL). Tests for serum EBV IgM antibodies and EBV early Antigen antibodies were positive, indicating acute EBV infection. Lymphocytosis resolved along with significant clinical improvement at the 10-day follow up visit. Even though patient did receive antibiotics, multiple factors including isolated lymphocytosis, pathology positive for EBV with no neutrophilia were more suggestive of sinusitis caused by viral infection, EBV in this case. Lymphocytosis with fever and sore throat should prompt physicians to consider IM. There are no known reports in the literature of EBV as a causal organism for acute viral sinusitis. There are some studies relating EBV with ENKTCL. It is unknown whether this particular patient with a history of EBV sinusitis will be at high risk for nasal type lymphoma in the future. Further studies should be conducted to understand the pathogenesis and relationship between EBV and ENKTCL.
Learning points: Infectious mononucleosis (IM) can present with various atypical presentations. Consideration of IM should not be limited to people presenting with a triad of fever, lymphadenopathy and sore throat. Lymphocytosis with atypical symptoms should raise suspicion of infectious mononucleosis.No case has been reported of EBV as a causal organism for acute sinusitis. Association with EBV infection and chronic sinusitis or nasal polyp or extranodal NK/T cell lymphoma has been demonstrated but pathogenesis is poorly understood.Studies should be done on whether acute sinusitis secondary to EBV poses a risk for nasal type lymphoma.
Keywords: Epstein Barr Infection; infectious mononucleosis; lymphocytosis; viral sinusitis.
© EFIM 2023.
Conflict of interest statement
Conflicts of Interests: The Authors declare that there are no competing interests.
Figures
References
-
- Joki-Erkkilä VP, Hietaharju A, Dastidar P, Numminen J, Puhakka H. Multiple cranial nerve palsies as a complication of infectious mononucleosis due to inflammatory lesion in jugular foramen. Ann Otol Rhinol Laryngol. 2000;109:340–342. - PubMed
-
- Tselis A, Duman R, Storch GA, Lisak RP. Epstein-Barr virus encephalomyelitis diagnosed by polymerase chain reaction: detection of the genome in the CSF. Neurology. 1997;48:1351–1355. - PubMed
-
- Ebell MH, Call M, Shinholser J, Gardner J. Does This Patient Have Infectious Mononucleosis? JAMA. 2016;315:1502. - PubMed
LinkOut - more resources
Full Text Sources