

This is a preprint.
Invasive neurophysiology and whole brain connectomics for neural decoding in patients with brain implants
- PMID: 37790428
- PMCID: PMC10543023
- DOI: 10.21203/rs.3.rs-3212709/v1
Invasive neurophysiology and whole brain connectomics for neural decoding in patients with brain implants
Update in
-
Invasive neurophysiology and whole brain connectomics for neural decoding in patients with brain implants.Nat Biomed Eng. 2025 Sep 24. doi: 10.1038/s41551-025-01467-9. Online ahead of print. Nat Biomed Eng. 2025. PMID: 40993190
Abstract
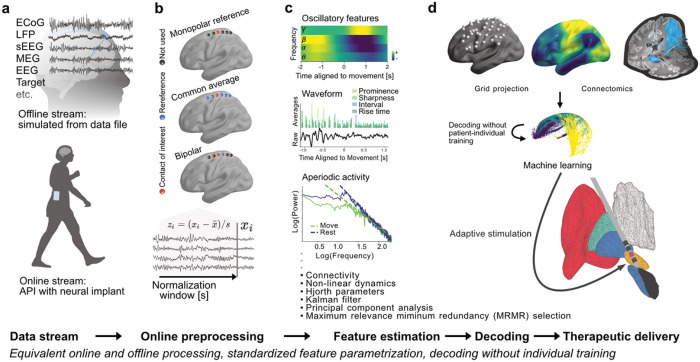
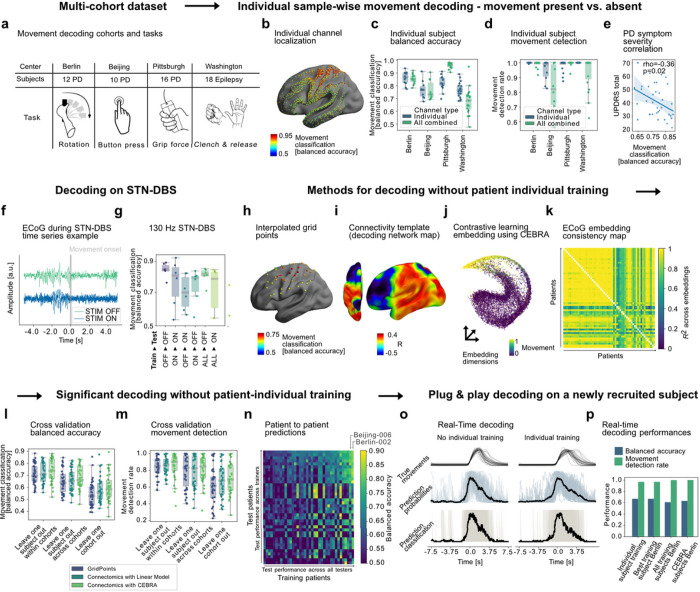
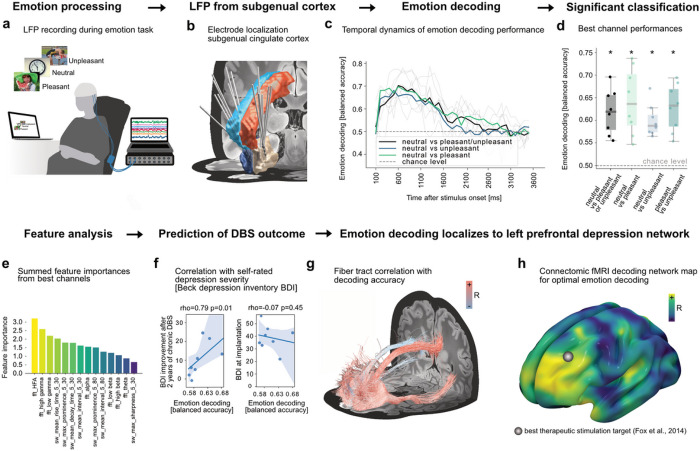
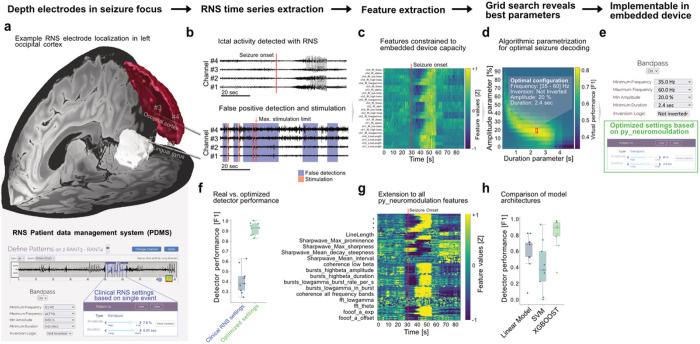
Brain computer interfaces (BCI) provide unprecedented spatiotemporal precision that will enable significant expansion in how numerous brain disorders are treated. Decoding dynamic patient states from brain signals with machine learning is required to leverage this precision, but a standardized framework for identifying and advancing novel clinical BCI approaches does not exist. Here, we developed a platform that integrates brain signal decoding with connectomics and demonstrate its utility across 123 hours of invasively recorded brain data from 73 neurosurgical patients treated for movement disorders, depression and epilepsy. First, we introduce connectomics-informed movement decoders that generalize across cohorts with Parkinson's disease and epilepsy from the US, Europe and China. Next, we reveal network targets for emotion decoding in left prefrontal and cingulate circuits in DBS patients with major depression. Finally, we showcase opportunities to improve seizure detection in responsive neurostimulation for epilepsy. Our platform provides rapid, high-accuracy decoding for precision medicine approaches that can dynamically adapt neuromodulation therapies in response to the individual needs of patients.
Figures
References
-
- Khambhati A. N., Shafi A., Rao V. R. & Chang E. F. Long-term brain network reorganization predicts responsive neurostimulation outcomes for focal epilepsy. Sci Transl Med 13, eabf6588 (2021). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
