

This is a preprint.
Complexities of cerebral small vessel disease, blood pressure, and dementia relationship: new insights from genetics
- PMID: 37790435
- PMCID: PMC10543241
- DOI: 10.1101/2023.08.08.23293761
Complexities of cerebral small vessel disease, blood pressure, and dementia relationship: new insights from genetics
Update in
-
Genetic Complexities of Cerebral Small Vessel Disease, Blood Pressure, and Dementia.JAMA Netw Open. 2024 May 1;7(5):e2412824. doi: 10.1001/jamanetworkopen.2024.12824. JAMA Netw Open. 2024. PMID: 38776079 Free PMC article.
Abstract
Importance: There is increasing recognition that vascular disease, which can be treated, is a key contributor to dementia risk. However, the contribution of specific markers of vascular disease is unclear and, as a consequence, optimal prevention strategies remain unclear.
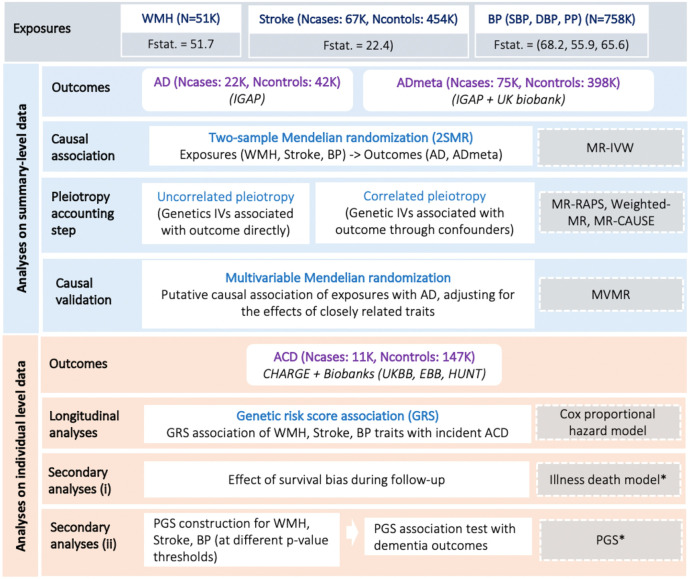
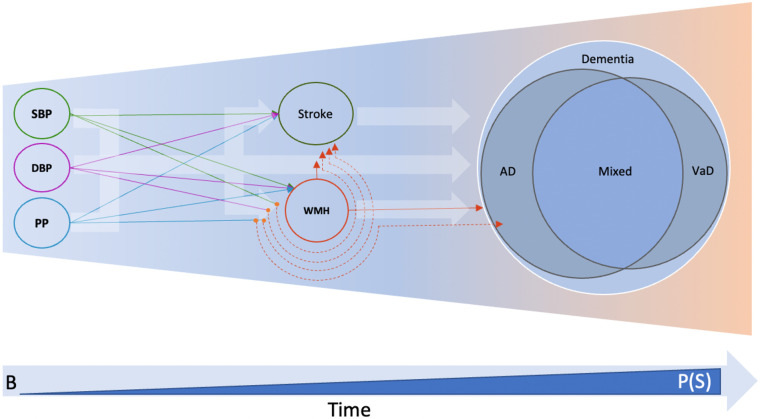
Objective: To disentangle the causal relation of several key vascular traits to dementia risk: (i) white matter hyperintensity (WMH) burden, a highly prevalent imaging marker of covert cerebral small vessel disease (cSVD); (ii) clinical stroke; and (iii) blood pressure (BP), the leading risk factor for cSVD and stroke, for which efficient therapies exist. To account for potential epidemiological biases inherent to late-onset conditions like dementia.
Design setting and participants: This study first explored the association of genetically determined WMH, BP levels and stroke risk with AD using summary-level data from large genome-wide association studies (GWASs) in a two-sample Mendelian randomization (MR) framework. Second, leveraging individual-level data from large longitudinal population-based cohorts and biobanks with prospective dementia surveillance, the association of weighted genetic risk scores (wGRSs) for WMH, BP, and stroke with incident all-cause-dementia was explored using Cox-proportional hazard and multi-state models. The data analysis was performed from July 26, 2020, through July 24, 2022.
Exposures: Genetically determined levels of WMH volume and BP (systolic, diastolic and pulse blood pressures) and genetic liability to stroke.
Main outcomes and measures: The summary-level MR analyses focused on the outcomes from GWAS of clinically diagnosed AD (n-cases=21,982) and GWAS additionally including self-reported parental history of dementia as a proxy for AD diagnosis (ADmeta, n-cases=53,042). For the longitudinal analyses, individual-level data of 157,698 participants with 10,699 incident all-cause-dementia were studied, exploring AD, vascular or mixed dementia in secondary analyses.
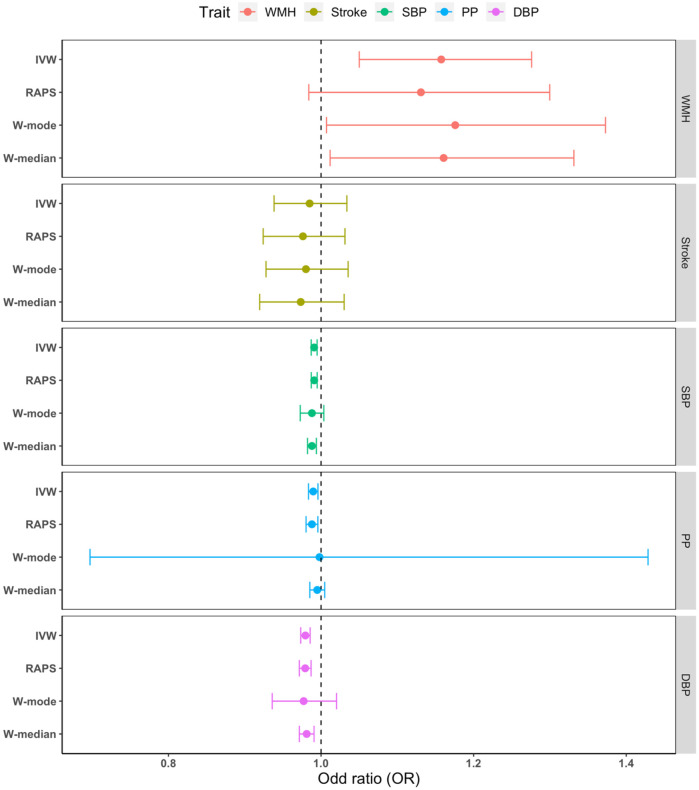
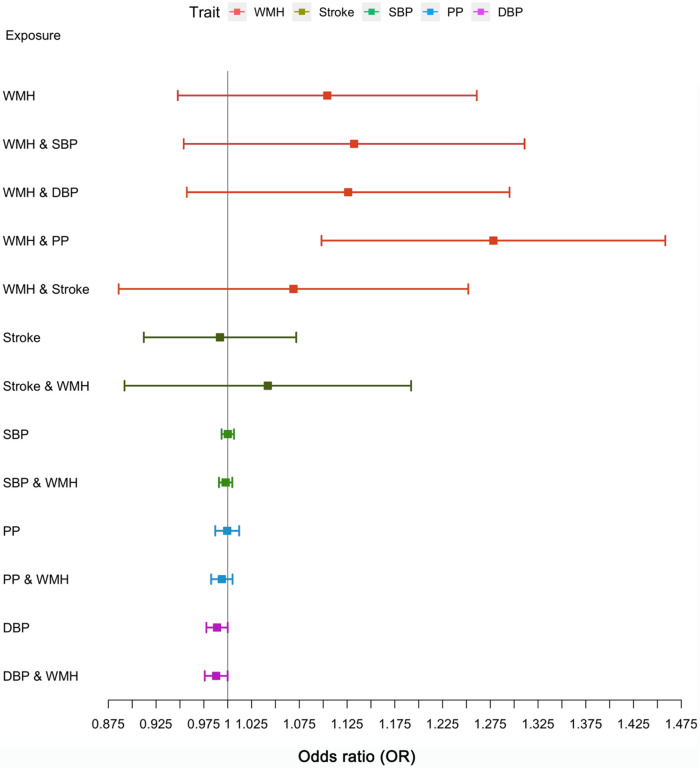
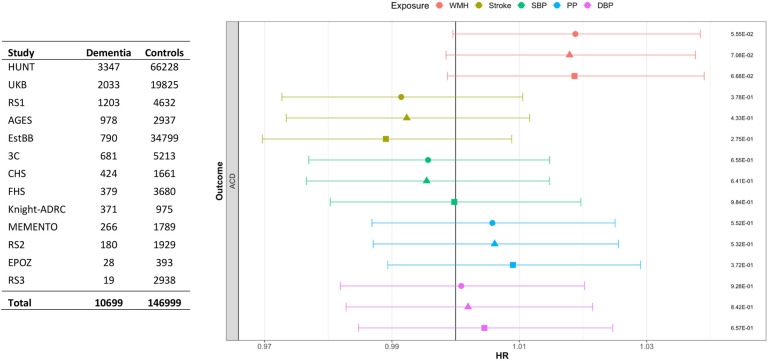
Results: In the two-sample MR analyses, WMH showed strong evidence for a causal association with increased risk of ADmeta (OR, 1.16; 95%CI:1.05-1.28; P=.003) and AD (OR, 1.28; 95%CI:1.07-1.53; P=.008), after accounting for genetically determined pulse pressure for the latter. Genetically predicted BP traits showed evidence for a protective association with both clinically defined AD and ADmeta, with evidence for confounding by shared genetic instruments. In longitudinal analyses the wGRSs for WMH, but not BP or stroke, showed suggestive association with incident all-cause-dementia (HR, 1.02; 95%CI:1.00-1.04; P=.06). BP and stroke wGRSs were strongly associated with mortality but there was no evidence for selective survival bias during follow-up. In secondary analyses, polygenic scores with more liberal instrument definition showed association of both WMH and stroke with all-cause-dementia, AD, and vascular or mixed dementia; associations of stroke, but not WMH, with dementia outcomes were markedly attenuated after adjusting for interim stroke.
Conclusion: These findings provide converging evidence that WMH is a leading vascular contributor to dementia risk, which may better capture the brain damage caused by BP (and other etiologies) than BP itself and should be targeted in priority for dementia prevention in the population.
Figures
References
-
- Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. The Lancet. 2016;388(10053):1459–1544. doi: 10.1016/S0140-6736(16)31012-1 - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources