

This is a preprint.
Nanoparticle delivery of innate immune agonists combines with senescence-inducing agents to mediate T cell control of pancreatic cancer
- PMID: 37790484
- PMCID: PMC10542133
- DOI: 10.1101/2023.09.18.558307
Nanoparticle delivery of innate immune agonists combines with senescence-inducing agents to mediate T cell control of pancreatic cancer
Update in
-
Nanoparticle delivery of innate immune agonists combined with senescence-inducing agents promotes T cell control of pancreatic cancer.Sci Transl Med. 2024 Aug 28;16(762):eadj9366. doi: 10.1126/scitranslmed.adj9366. Epub 2024 Aug 28. Sci Transl Med. 2024. PMID: 39196958 Free PMC article.
Abstract
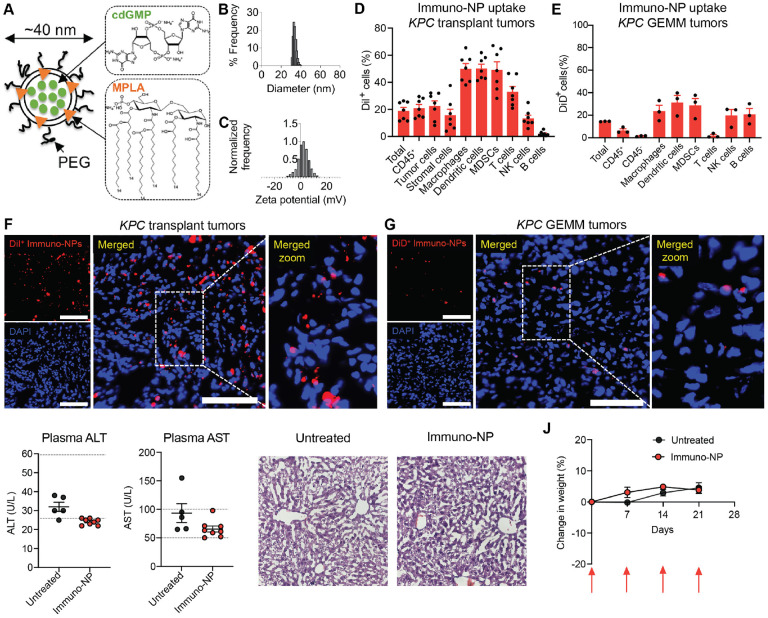
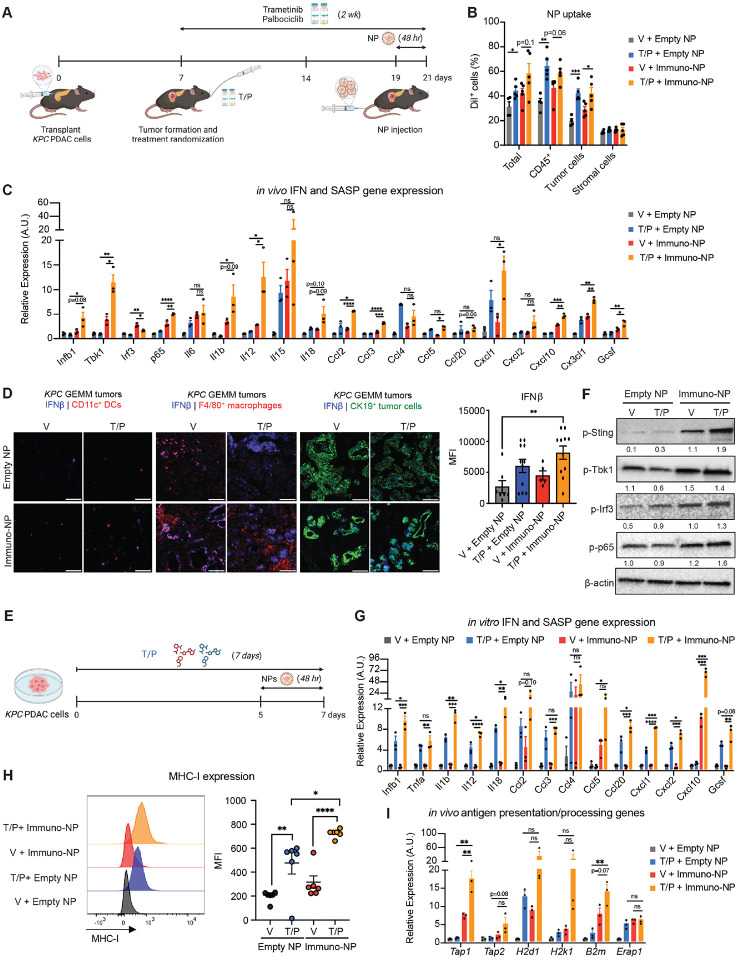
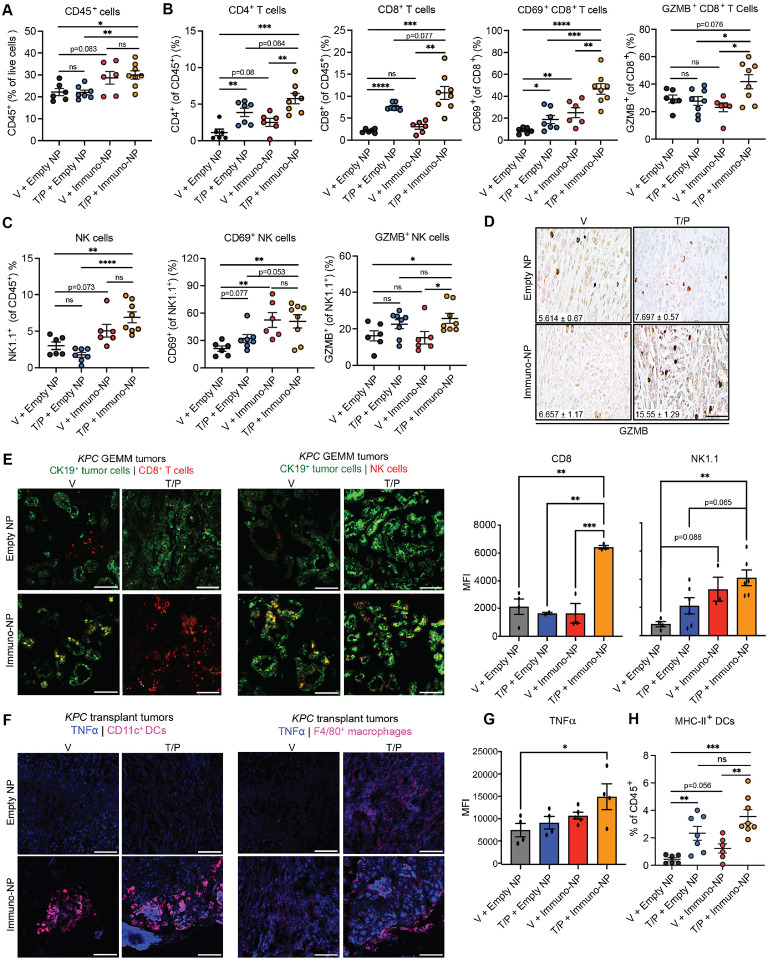
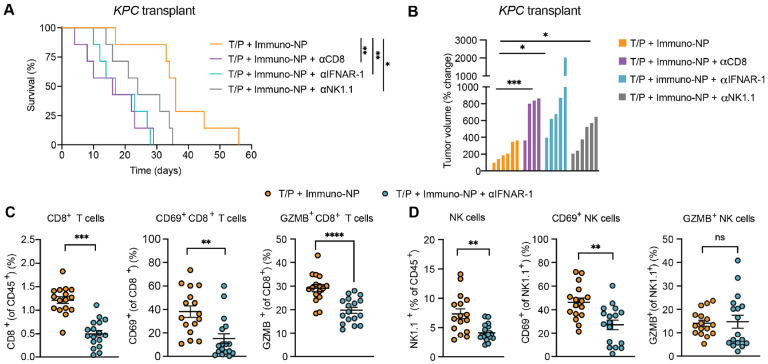
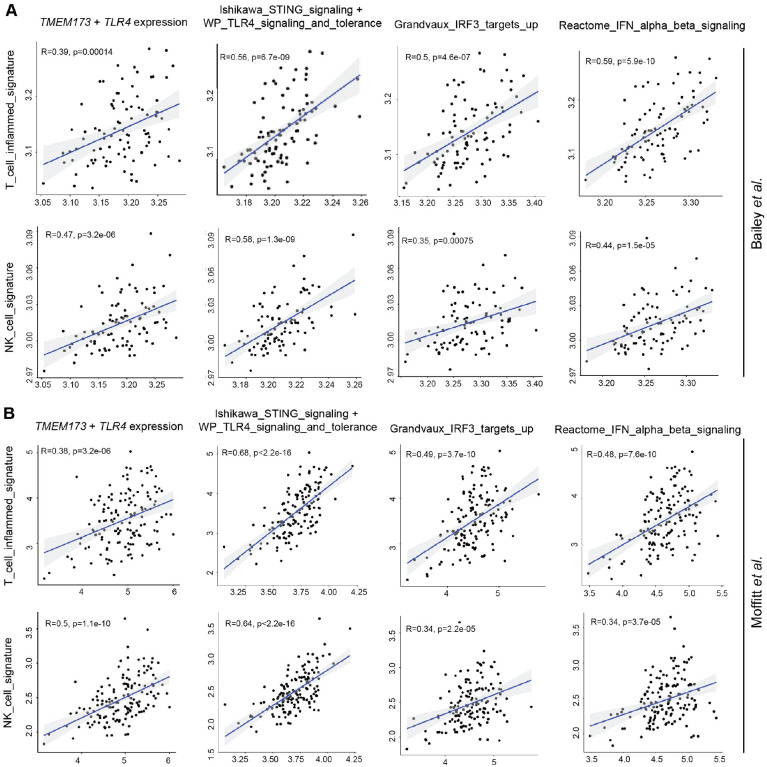
Pancreatic ductal adenocarcinoma has quickly risen to become the 3rd leading cause of cancer-related death. This is in part due to its fibrotic tumor microenvironment (TME) that contributes to poor vascularization and immune infiltration and subsequent chemo- and immunotherapy failure. Here we investigated an innovative immunotherapy approach combining local delivery of STING and TLR4 innate immune agonists via lipid-based nanoparticles (NPs) co-encapsulation with senescence-inducing RAS-targeted therapies that can remodel the immune suppressive PDAC TME through the senescence-associated secretory phenotype. Treatment of transplanted and autochthonous PDAC mouse models with these regimens led to enhanced uptake of NPs by multiple cell types in the PDAC TME, induction of type I interferon and other pro-inflammatory signaling, increased antigen presentation by tumor cells and antigen presenting cells, and subsequent activation of both innate and adaptive immune responses. This two-pronged approach produced potent T cell-driven and Type I interferon-dependent tumor regressions and long-term survival in preclinical PDAC models. STING and TLR4-mediated Type I interferon signaling were also associated with enhanced NK and CD8+ T cell immunity in human PDAC. Thus, combining localized immune agonist delivery with systemic tumor-targeted therapy can synergize to orchestrate a coordinated innate and adaptive immune assault to overcome immune suppression and activate durable anti-tumor T cell responses against PDAC.
Conflict of interest statement
Competing Interests: M.R. is a consultant for Boehringer Ingelheim. L.C., G.I.K., P.U.A., and M.R. have filed a U.S. patent application (Ser. No. 63/466,164) related to this work. The other authors declare no competing interests.
Figures

References
-
- Siegel R. L., Miller K. D., Wagle N. S., Jemal A., Cancer statistics, 2023. CA Cancer J Clin 73, 17–48 (2023). - PubMed
-
- Brahmer J. R., Tykodi S. S., Chow L. Q., Hwu W. J., Topalian S. L., Hwu P., Drake C. G., Camacho L. H., Kauh J., Odunsi K., Pitot H. C., Hamid O., Bhatia S., Martins R., Eaton K., Chen S., Salay T. M., Alaparthy S., Grosso J. F., Korman A. J., Parker S. M., Agrawal S., Goldberg S. M., Pardoll D. M., Gupta A., Wigginton J. M., Safety and activity of anti-PD-L1 antibody in patients with advanced cancer. N Engl J Med 366, 2455–2465 (2012). - PMC - PubMed
-
- Royal R. E., Levy C., Turner K., Mathur A., Hughes M., Kammula U. S., Sherry R. M., Topalian S. L., Yang J. C., Lowy I., Rosenberg S. A., Phase 2 trial of single agent Ipilimumab (anti-CTLA-4) for locally advanced or metastatic pancreatic adenocarcinoma. J Immunother 33, 828–833 (2010). - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous