

Ongoing substrate-driven atrial fibrillation "boxed" in the left atrial posterior wall with ablation: a case report
- PMID: 37790595
- PMCID: PMC10542893
- DOI: 10.3389/fcvm.2023.1251874
Ongoing substrate-driven atrial fibrillation "boxed" in the left atrial posterior wall with ablation: a case report
Abstract
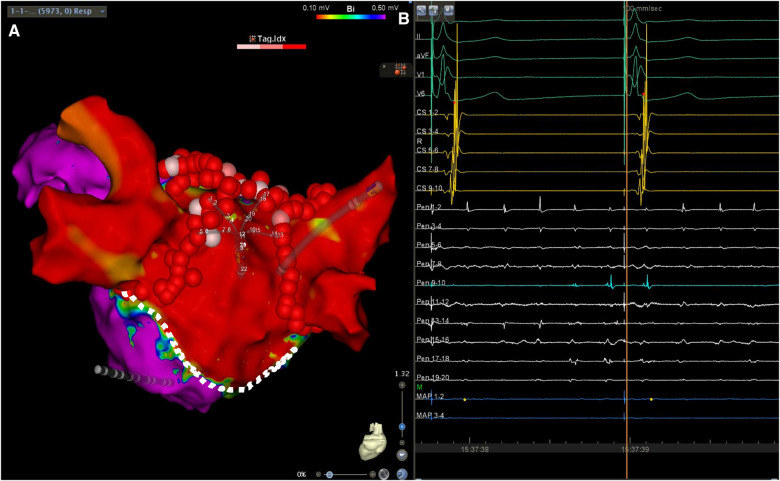
Patients undergoing valve surgery for rheumatic heart disease are expected to develop significant atrial arrhythmogenic substrates outside of the pulmonary veins, which sometimes require complex ablation techniques for the treatment of symptomatic arrhythmias. We describe, herein, the case of a 76-year-old male undergoing endocardial ablation for the treatment of symptomatic persistent atrial fibrillation which developed after aortic and mitral valve replacement with a simultaneous tricuspid ring annuloplasty. Following pulmonary vein isolation, the patient's atrial fibrillation was converted into cavotricuspid isthmus-dependent atrial flutter. After a successful cavotricuspid isthmus ablation, the arrhythmia reverted back to a left atrial tachyarrhythmia originating from the posterior wall. A linear left atrial lesion led to the electrical isolation of a large area, which included the posterior wall, as well as the containment of the ongoing fibrillatory activity, while sinus rhythm was restored in the rest of the atria. In conclusion, successful left atrial posterior wall isolation can be achieved in the setting of severe scarring due to previous atriotomy by creating a linear lesion on the atrial roof, in conjunction with pulmonary vein isolation, sparing the patient from requiring bottom-line ablation, and avoiding possible esophageal injury. Such compartmentalization of the left atrium may effectively contain local fibrillatory activity, while allowing for the restoration of sinus rhythm.
Keywords: ablation; box lesion; case report; independent tachycardia; posterior wall.
© 2023 Traykov, Marchov, Martinov, El Abbady, Gelev and Dichtl.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Rodríguez-Mañero M, Valderrábano M, Baluja A, Kreidieh O, Martínez-Sande J, García-Seara J, et al. Validating left atrial low voltage areas during atrial fibrillation and atrial flutter using multielectrode automated electroanatomic mapping. JACC Clin Electrophysiol. (2018) 4(12):1541–52. 10.1016/j.jacep.2018.08.015 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources