

Carpal Tunnel Release With Ultrasound Guidance: Intermediate-Term Clinical Outcomes and Magnetic Resonance Imaging Findings
- PMID: 37790816
- PMCID: PMC10543793
- DOI: 10.1016/j.jhsg.2023.05.002
Carpal Tunnel Release With Ultrasound Guidance: Intermediate-Term Clinical Outcomes and Magnetic Resonance Imaging Findings
Abstract
Purpose: The purpose of this study was to report intermediate-term outcomes following carpal tunnel release using ultrasound guidance and wide-awake local anesthesia no tourniquet, including a subset of patients with preoperative and postoperative magnetic resonance imaging (MRI).
Methods: In this observational study, patients with carpal tunnel syndrome were treated with carpal tunnel release using ultrasound guidance and wide-awake local anesthesia no tourniquet in a procedure room at a single center. Main outcomes were complications; return to activity and work at 2 weeks; Quick Disabilities of the Arm, Shoulder, and Hand and Boston Carpal Tunnel Questionnaire scores through 6 months; and postoperative morphological changes of the transverse carpal ligament, median nerve, and carpal tunnel evaluated using MRI.
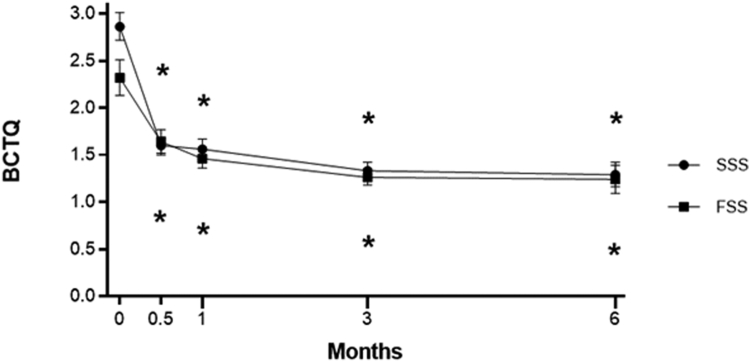
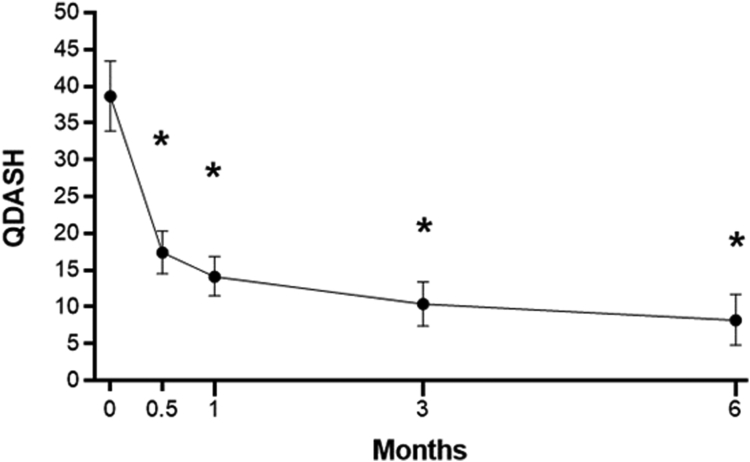
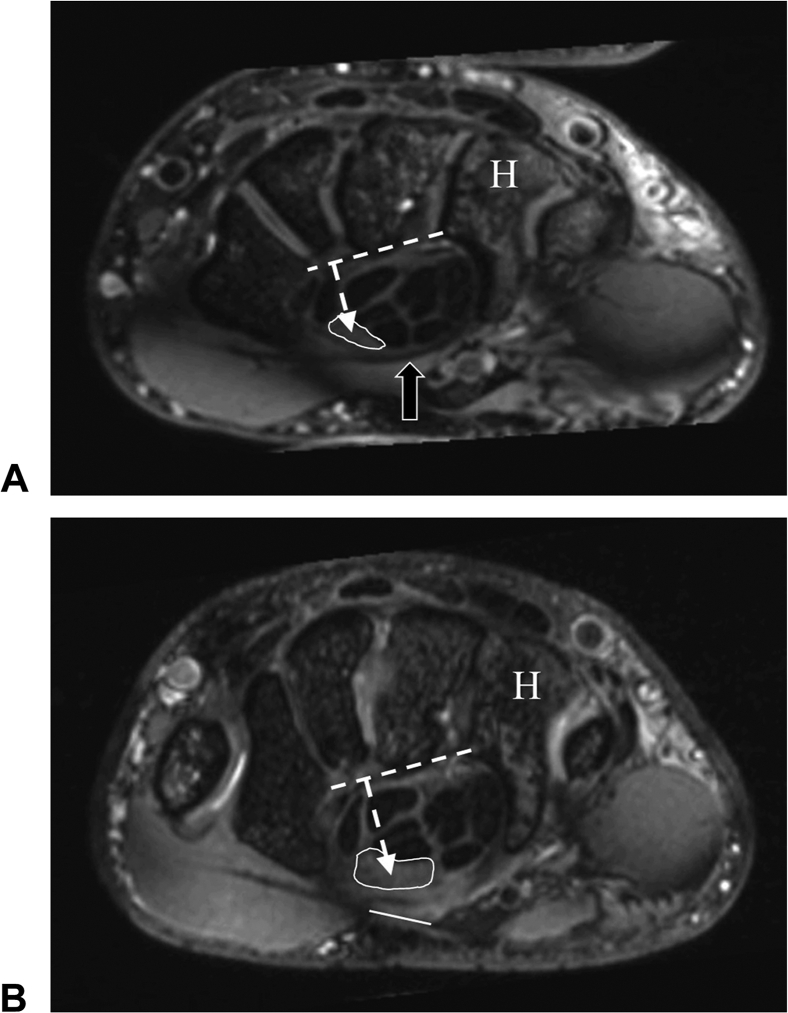
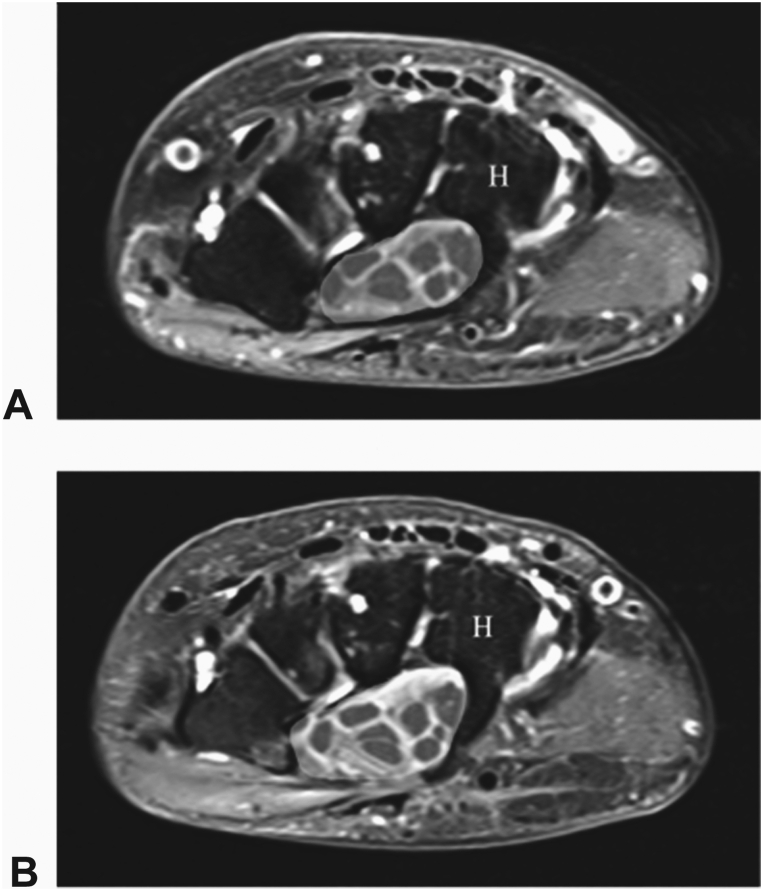
Results: No complications were reported among 65 patients (68% women, 96 wrists). By 2 weeks, 97% of patients returned to normal activity and 100% returned to work. Statistically significant improvements in Boston Carpal Tunnel Questionnaire symptom severity scale, Boston Carpal Tunnel Questionnaire functional status scale, and Quick Disabilities of the Arm, Shoulder, and Hand scores occurred by the 2-week follow-up interval and persisted at 6 months (all P < .001). Pre- and postoperative MRI scans were available for 13 patients (17 wrists) at the 3-month mean follow-up. Complete transverse carpal ligament transection was documented in all wrists. Key MRI findings included a 22% increase in carpal tunnel cross-sectional area at the hamate (P < .001), a 52% increase in median nerve cross-sectional area at the hamate (P < .001), an 18% reduction in median nerve signal intensity (P = .002), a 38% reduction in the flattening ratio of the median nerve at the hamate (P < .001), a 33% reduction in the flattening ratio of the median nerve at the pisiform (P < .001), a 20% reduction in the flattening ratio of the carpal tunnel at the hamate (P < .001), and a palmar shift of the median nerve relative to the hamate in all cases.
Conclusions: Carpal tunnel release using ultrasound guidance using wide-awake local anesthesia no tourniquet in a procedure room setting was safe, effective, and resulted in morphological changes that were consistent with carpal tunnel decompression as demonstrated by MRI.
Type of study/level of evidence: Therapeutic IV.
Keywords: CTR-US; Carpal tunnel release; Carpal tunnel syndrome; Magnetic resonance imaging; WALANT.
© 2023 The Authors.
Figures
Similar articles
-
Median nerve compression can be detected by magnetic resonance imaging of the carpal tunnel.Neurosurgery. 1997 Jul;41(1):76-82; discussion 82-3. doi: 10.1097/00006123-199707000-00016. Neurosurgery. 1997. PMID: 9218298
-
Minimally Invasive Ultrasound-Guided Carpal Tunnel Release Improves Long-Term Clinical Outcomes in Carpal Tunnel Syndrome.AJR Am J Roentgenol. 2021 Aug;217(2):460-468. doi: 10.2214/AJR.20.24383. Epub 2020 Sep 2. AJR Am J Roentgenol. 2021. PMID: 32876476
-
The pressure angle of the median nerve as a new magnetic resonance imaging parameter for the evaluation of carpal tunnel.Clin Neurol Neurosurg. 2009 Jan;111(1):28-33. doi: 10.1016/j.clineuro.2008.07.008. Epub 2008 Oct 9. Clin Neurol Neurosurg. 2009. PMID: 18848388
-
Carpal Tunnel Release without a Tourniquet: A Systematic Review and Meta-Analysis.Plast Reconstr Surg. 2020 Mar;145(3):737-744. doi: 10.1097/PRS.0000000000006549. Plast Reconstr Surg. 2020. PMID: 32097317
-
Ultrasound-guided release of carpal tunnel syndrome - Anterograde technique.Hand Surg Rehabil. 2025 May;44S:102091. doi: 10.1016/j.hansur.2025.102091. Epub 2025 Jan 21. Hand Surg Rehabil. 2025. PMID: 39848544 Review.
Cited by
-
Carpal Tunnel Release with Ultrasound Guidance Versus Open and Mini-Open Carpal Tunnel Release: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.J Hand Surg Glob Online. 2025 Jan 20;7(2):121-126. doi: 10.1016/j.jhsg.2024.04.001. eCollection 2025 Mar. J Hand Surg Glob Online. 2025. PMID: 40182888 Free PMC article.
-
Long-Term Clinical Results of Carpal Tunnel Release Using Ultrasound Guidance: A Multicenter Pragmatic Study.J Hand Surg Glob Online. 2023 Nov 22;6(1):79-84. doi: 10.1016/j.jhsg.2023.10.001. eCollection 2024 Jan. J Hand Surg Glob Online. 2023. PMID: 38313613 Free PMC article.
References
-
- Atroshi I., Englund M., Turkiewicz A., Tägil M., Petersson I.F. Incidence of physician-diagnosed carpal tunnel syndrome in the general population. Arch Intern Med. 2011;171(10):943–944. - PubMed
-
- Palmer D.H., Hanrahan L.P. Social and economic costs of carpal tunnel surgery. Instr Course Lect. 1995;44:167–172. - PubMed
-
- Fowler J.R., Chung K.C., Miller L.E. Multicenter pragmatic study of carpal tunnel release with ultrasound guidance. Expert Rev Med Devices. 2022;19(3):273–280. - PubMed
-
- Okutsu I., Ninomiya S., Takatori Y., Ugawa Y. Endoscopic management of carpal tunnel syndrome. Arthroscopy. 1989;5(1):11–18. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
