

Associations Between Rheumatoid Arthritis Clinical Factors and Synovial Cell Types and States
- PMID: 37791989
- PMCID: PMC10922423
- DOI: 10.1002/art.42726
Associations Between Rheumatoid Arthritis Clinical Factors and Synovial Cell Types and States
Abstract
Objective: Recent studies have uncovered diverse cell types and states in the rheumatoid arthritis (RA) synovium; however, limited data exist correlating these findings with patient-level clinical information. Using the largest cohort to date with clinical and multicell data, we determined associations between RA clinical factors with cell types and states in the RA synovium.
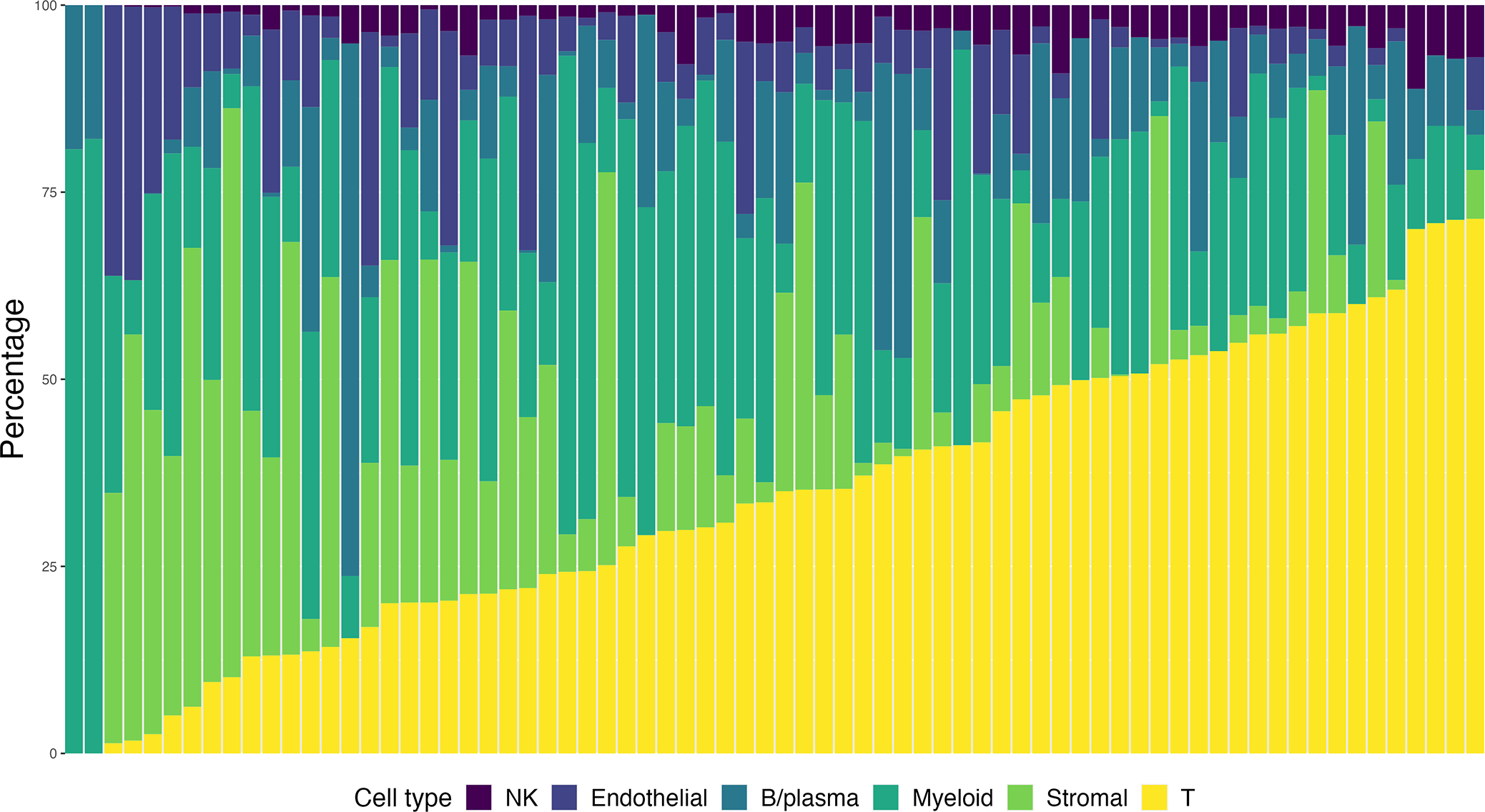
Methods: The Accelerated Medicines Partnership Rheumatoid Arthritis study recruited patients with active RA who were not receiving disease-modifying antirheumatic drugs (DMARDs) or who had an inadequate response to methotrexate (MTX) or tumor necrosis factor inhibitors. RA clinical factors were systematically collected. Biopsies were performed on an inflamed joint, and tissue were disaggregated and processed with a cellular indexing of transcriptomes and epitopes sequencing pipeline from which the following cell type percentages and cell type abundance phenotypes (CTAPs) were derived: endothelial, fibroblast, and myeloid (EFM); fibroblasts; myeloid; T and B cells; T cells and fibroblasts (TF); and T and myeloid cells. Correlations were measured between RA clinical factors, cell type percentage, and CTAPs.
Results: We studied 72 patients (mean age 57 years, 75% women, 83% seropositive, mean RA duration 6.6 years, mean Disease Activity Score-28 C-reactive Protein 3 [DAS28-CRP3] score 4.8). Higher DAS28-CRP3 correlated with a higher T cell percentage (P < 0.01). Those receiving MTX and not a biologic DMARD (bDMARD) had a higher percentage of B cells versus those receiving no DMARDs (P < 0.01). Most of those receiving bDMARDs were categorized as EFM (57%), whereas none were TF. No significant difference was observed across CTAPs for age, sex, RA disease duration, or DAS28-CRP3.
Conclusion: In this comprehensive screen of clinical factors, we observed differential associations between DMARDs and cell phenotypes, suggesting that RA therapies, more than other clinical factors, may impact cell type/state in the synovium and ultimately influence response to subsequent therapies.
© 2023 American College of Rheumatology.
Conflict of interest statement
Competing interests
A.H.J. reports research support from Amgen, outside the submitted work. K.W. is a consultant for Mestag Therapeutics and Gilead Sciences and reports grant support from Gilead Sciences. S.G. reports research support from Novartis and is a consultant for UCB, outside the submitted work. V.M.H. is a co-founder of Q32 Bio and has previously received sponsored research from Janssen and been a consultant for Celgene and BMS, outside the submitted work. A.F. reports personal fees from Abbvie, Roche, and Janssen and grant support from Roche, UCB, Nascient, Mestag, GlaxoSmithKline, and Janssen, outside the submitted work. D.A.R. reports personal fees from Pfizer, Janssen, Merck, Scipher Medicine, GlaxoSmithKline, and Bristol-Myers Squibb and grant support from Janssen and Bristol-Myers Squibb, outside the submitted work. In addition, D.A.R. is a co-inventor on a patent submitted on T peripheral helper cells. M.B. is a founder for Mestag Therapeutics and a consultant for GlaxoSmithKline, 4FO Ventures, and Scailyte AG. S.R. is a founder for Mestag Therapeutics, a scientific advisor for Janssen and Pfizer, and a consultant for Gilead and Rheos Medicines.
Figures

References
MeSH terms
Substances
Grants and funding
- UH2AR067676/AR/NIAMS NIH HHS/United States
- UH2 AR067685/AR/NIAMS NIH HHS/United States
- U01HG009379/HG/NHGRI NIH HHS/United States
- UH2 AR067681/AR/NIAMS NIH HHS/United States
- UH2AR067689/AR/NIAMS NIH HHS/United States
- UH2 AR067689/AR/NIAMS NIH HHS/United States
- UH2AR067691/AR/NIAMS NIH HHS/United States
- K08 AR077037/AR/NIAMS NIH HHS/United States
- R01 AI148435/AI/NIAID NIH HHS/United States
- UH2AR067690/AR/NIAMS NIH HHS/United States
- R01AR063759/AR/NIAMS NIH HHS/United States
- R01AR073290/AR/NIAMS NIH HHS/United States
- P30AR069655/AR/NIAMS NIH HHS/United States
- UH2AR067694/AR/NIAMS NIH HHS/United States
- UM2 AR067678/AR/NIAMS NIH HHS/United States
- P30 AR069655/AR/NIAMS NIH HHS/United States
- R21 AR071670/AR/NIAMS NIH HHS/United States
- K08 AR081412/AR/NIAMS NIH HHS/United States
- P30 AR072577/AR/NIAMS NIH HHS/United States
- UH2AR067677/AR/NIAMS NIH HHS/United States
- MR/M007669/1/MRC_/Medical Research Council/United Kingdom
- R01 AR073290/AR/NIAMS NIH HHS/United States
- UH2AR067679/AR/NIAMS NIH HHS/United States
- T32 HG002295/HG/NHGRI NIH HHS/United States
- R01AR073833/AR/NIAMS NIH HHS/United States
- R01 AR073833/AR/NIAMS NIH HHS/United States
- UH2AR067688/AR/NIAMS NIH HHS/United States
- MR/P021220/1/MRC_/Medical Research Council/United Kingdom
- UH2 AR067688/AR/NIAMS NIH HHS/United States
- K08 AR072791/AR/NIAMS NIH HHS/United States
- K08AR072791/AR/NIAMS NIH HHS/United States
- P30AR072577/AR/NIAMS NIH HHS/United States
- UM2AR067678/AR/NIAMS NIH HHS/United States
- R01 AR063759/AR/NIAMS NIH HHS/United States
- UH2 AR067690/AR/NIAMS NIH HHS/United States
- UH2AR067681/AR/NIAMS NIH HHS/United States
- UH2 AR067677/AR/NIAMS NIH HHS/United States
- R21AR071670/AR/NIAMS NIH HHS/United States
- U01 HG009379/HG/NHGRI NIH HHS/United States
- UH2AR067685/AR/NIAMS NIH HHS/United States
- UH2 AR067694/AR/NIAMS NIH HHS/United States
- UH2 AR067679/AR/NIAMS NIH HHS/United States
- K08AR077037/AR/NIAMS NIH HHS/United States
- UH2 AR067676/AR/NIAMS NIH HHS/United States
- UH2 AR067691/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
