

Incidence change of postoperative delirium after implementation of processed electroencephalography monitoring during surgery: a retrospective evaluation study
- PMID: 37794315
- PMCID: PMC10548752
- DOI: 10.1186/s12871-023-02293-9
Incidence change of postoperative delirium after implementation of processed electroencephalography monitoring during surgery: a retrospective evaluation study
Abstract
Background: Postoperative delirium (POD) is a common complication in the elderly, which is associated with poor outcomes after surgery. Recognized as predisposing factors for POD, anesthetic exposure and burst suppression during general anesthesia can be minimized with intraoperative processed electroencephalography (pEEG) monitoring. In this study, we aimed to evaluate whether implementation of intraoperative pEEG-guided anesthesia is associated with incidence change of POD.
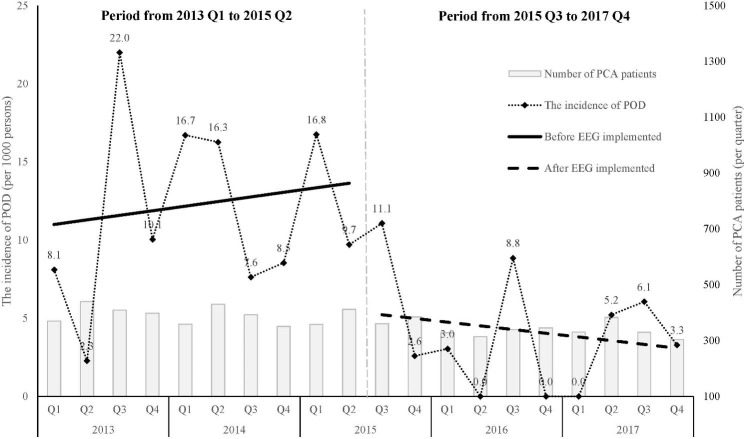
Methods: In this retrospective evaluation study, we analyzed intravenous patient-controlled analgesia (IVPCA) dataset from 2013 to 2017. There were 7425 patients using IVPCA after a noncardiac procedure under general anesthesia. Patients incapable of operating the device independently, such as cognitive dysfunction or prolonged sedation, were declined and not involved in the dataset. After excluding patients who opted out within three days (N = 110) and those with missing data (N = 24), 7318 eligible participants were enrolled. Intraoperative pEEG has been implemented since July 2015. Participants having surgery after this time point had intraoperative pEEG applied before induction until full recovery. All related staff had been trained in the application of pEEG-guided anesthesia and the assessment of POD. Patients were screened twice daily for POD within 3 days after surgery by staff in the pain management team. In the first part of this study, we compared the incidence of POD and its trend from 2013 January-2015 July with 2015 July-2017 December. In the second part, we estimated odds ratios of risk factors for POD using multivariable logistic regression in case-control setting.
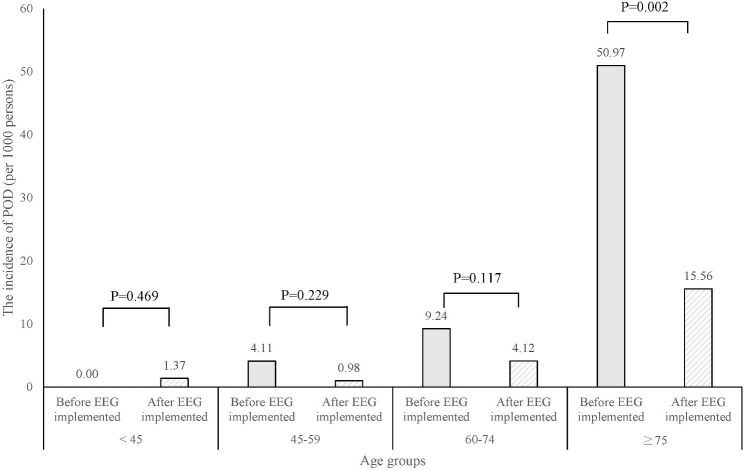
Results: The incidence of POD decreased from 1.18 to 0.41% after the administration of intraoperative pEEG. For the age group ≧ 75 years, POD incidence decreased from 5.1 to 1.56%. Further analysis showed that patients with pEEG-guided anesthesia were associated with a lower odd of POD (aOR 0.33; 95% CI 0.18-0.60) than those without after adjusting for other covariates.
Conclusions: Implementation of intraoperative pEEG was associated with a lower incidence of POD within 3 days after surgery, particularly in the elderly. Intraoperative pEEG might be reasonably considered as part of the strategy to prevent POD in the elder population.
Trial registration: Not applicable.
Keywords: General anesthesia; Intravenous patient-controlled analgesia; Postoperative delirium; Processed electroencephalography.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Electroencephalography-Guided Anesthesia and Delirium in Older Adults After Cardiac Surgery: The ENGAGES-Canada Randomized Clinical Trial.JAMA. 2024 Jul 9;332(2):112-123. doi: 10.1001/jama.2024.8144. JAMA. 2024. PMID: 38857019 Free PMC article. Clinical Trial.
-
Diurnal variation of postoperative delirium in elderly patients undergoing esketamine anesthesia for elective noncardiac surgery: a randomized clinical trial.Int J Surg. 2024 Sep 1;110(9):5496-5504. doi: 10.1097/JS9.0000000000001642. Int J Surg. 2024. PMID: 39275772 Free PMC article. Clinical Trial.
-
Lower alpha frequency of intraoperative frontal EEG is associated with postoperative delirium: A secondary propensity-matched analysis.J Clin Anesth. 2024 May;93:111343. doi: 10.1016/j.jclinane.2023.111343. Epub 2023 Nov 22. J Clin Anesth. 2024. PMID: 37995609
-
Perioperative Factors Associated With Postoperative Delirium in Patients Undergoing Noncardiac Surgery: An Individual Patient Data Meta-Analysis.JAMA Netw Open. 2023 Oct 2;6(10):e2337239. doi: 10.1001/jamanetworkopen.2023.37239. JAMA Netw Open. 2023. PMID: 37819663 Free PMC article.
-
Neuraxial versus general anesthesia in elderly patients undergoing hip fracture surgery and the incidence of postoperative delirium: a systematic review and stratified meta-analysis.BMC Anesthesiol. 2023 Jul 22;23(1):250. doi: 10.1186/s12871-023-02196-9. BMC Anesthesiol. 2023. PMID: 37481517 Free PMC article.
Cited by
-
Advances in research on the pathogenesis and signaling pathways associated with postoperative delirium (Review).Mol Med Rep. 2025 Aug;32(2):220. doi: 10.3892/mmr.2025.13585. Epub 2025 Jun 6. Mol Med Rep. 2025. PMID: 40476568 Free PMC article. Review.
References
-
- Anastasian ZH, Gaudet JG. 1 - Effects of Anesthetics, Operative Pharmacotherapy, and Recovery from Anesthesia. In: Neurocritical Care Management of the Neurosurgical Patient edn. Edited by Kumar M, Kofke WA, Levine JM, Schuster J. London: Elsevier; 2018: 3–14.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
