

Serum methylation of GALNT9, UPF3A, WARS, and LDB2 as noninvasive biomarkers for the early detection of colorectal cancer and advanced adenomas
- PMID: 37794510
- PMCID: PMC10552320
- DOI: 10.1186/s13148-023-01570-1
Serum methylation of GALNT9, UPF3A, WARS, and LDB2 as noninvasive biomarkers for the early detection of colorectal cancer and advanced adenomas
Abstract
Background: Early detection has proven to be the most effective strategy to reduce the incidence and mortality of colorectal cancer (CRC). Nevertheless, most current screening programs suffer from low participation rates. A blood test may improve both the adherence to screening and the selection to colonoscopy. In this study, we conducted a serum-based discovery and validation of cfDNA methylation biomarkers for CRC screening in a multicenter cohort of 433 serum samples including healthy controls, benign pathologies, advanced adenomas (AA), and CRC.
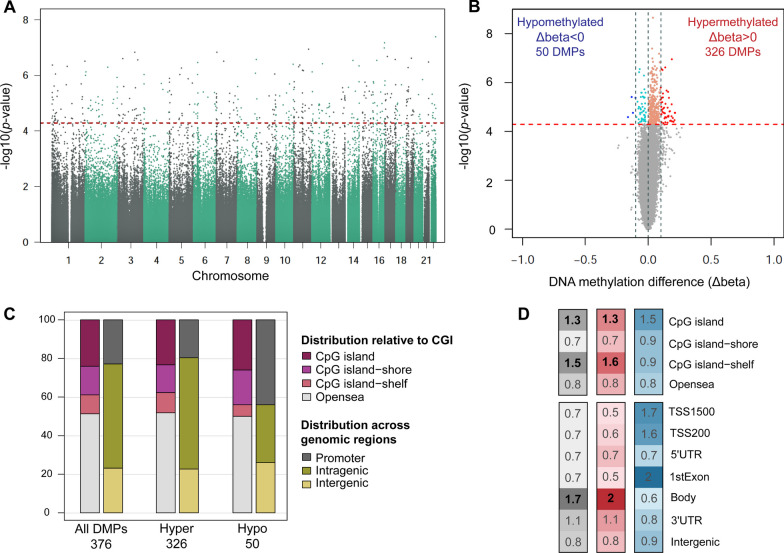
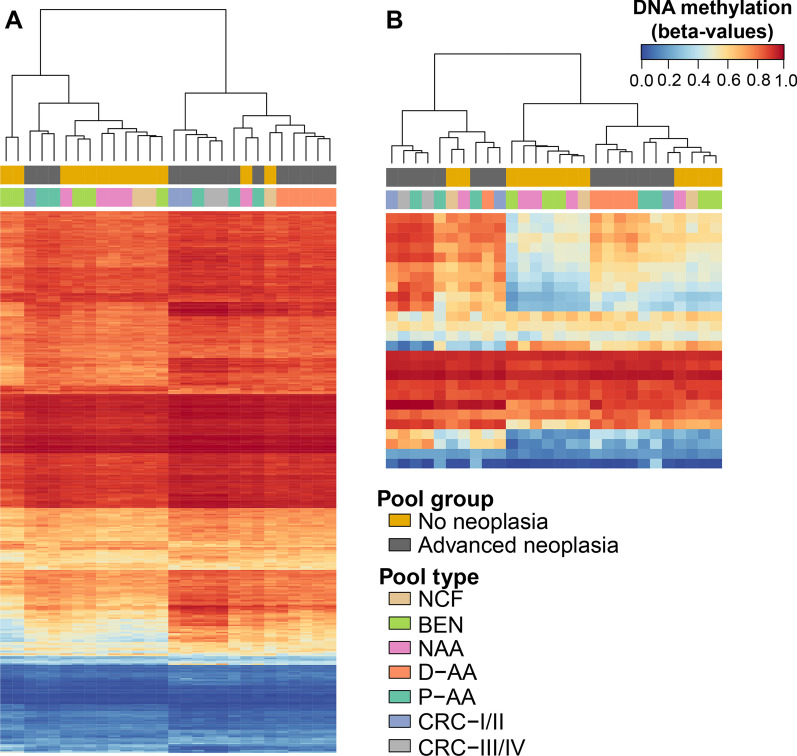
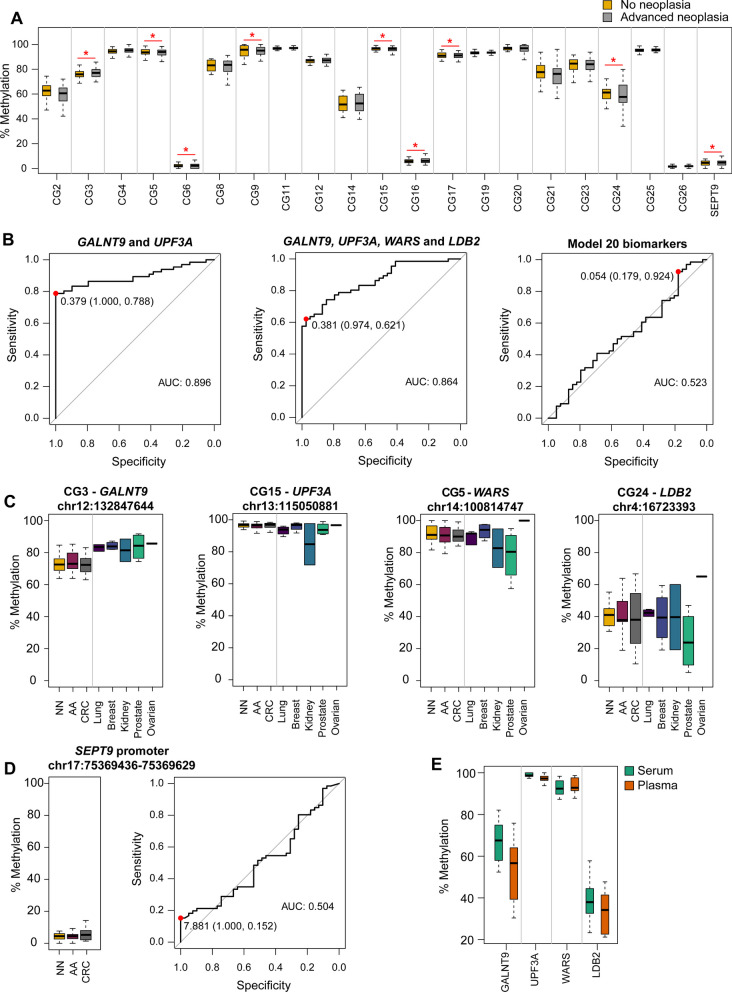
Results: First, we performed an epigenome-wide methylation analysis with the MethylationEPIC array using a sample pooling approach, followed by a robust prioritization of candidate biomarkers for the detection of advanced neoplasia (AN: AA and CRC). Then, candidate biomarkers were validated by pyrosequencing in independent individual cfDNA samples. We report GALNT9, UPF3A, WARS, and LDB2 as new noninvasive biomarkers for the early detection of AN. The combination of GALNT9/UPF3A by logistic regression discriminated AN with 78.8% sensitivity and 100% specificity, outperforming the commonly used fecal immunochemical test and the methylated SEPT9 blood test.
Conclusions: Overall, this study highlights the utility of cfDNA methylation for CRC screening. Our results suggest that the combination methylated GALNT9/UPF3A has the potential to serve as a highly specific and sensitive blood-based test for screening and early detection of CRC.
Keywords: Advanced adenomas; Cancer prevention; Circulating cell-free DNA; Colorectal cancer; DNA methylation; Liquid biopsy; Screening; Serum.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
