Severe autoimmune hemolytic anemia; epidemiology, clinical management, outcomes and knowledge gaps
- PMID: 37795092
- PMCID: PMC10545865
- DOI: 10.3389/fimmu.2023.1228142
Severe autoimmune hemolytic anemia; epidemiology, clinical management, outcomes and knowledge gaps
Abstract
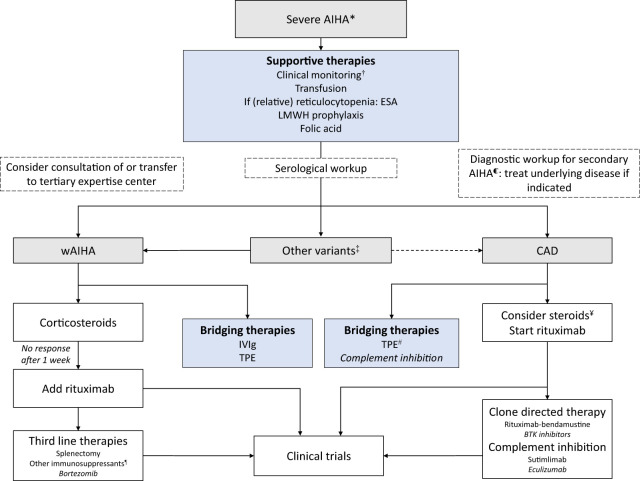
Autoimmune hemolytic anemia (AIHA) is an acquired hemolytic disorder, mediated by auto-antibodies, and has a variable clinical course ranging from fully compensated low grade hemolysis to severe life-threatening cases. The rarity, heterogeneity and incomplete understanding of severe AIHA complicate the recognition and management of severe cases. In this review, we describe how severe AIHA can be defined and what is currently known of the severity and outcome of AIHA. There are no validated predictors for severe clinical course, but certain risk factors for poor outcomes (hospitalisation, transfusion need and mortality) can aid in recognizing severe cases. Some serological subtypes of AIHA (warm AIHA with complement positive DAT, mixed, atypical) are associated with lower hemoglobin levels, higher transfusion need and mortality. Currently, there is no evidence-based therapeutic approach for severe AIHA. We provide a general approach for the management of severe AIHA patients, incorporating monitoring, supportive measures and therapeutic options based on expert opinion. In cases where steroids fail, there is a lack of rapidly effective therapeutic options. In this era, numerous novel therapies are emerging for AIHA, including novel complement inhibitors, such as sutimlimab. Their potential in severe AIHA is discussed. Future research efforts are needed to gain a clearer picture of severe AIHA and develop prediction models for severe disease course. It is crucial to incorporate not only clinical characteristics but also biomarkers that are associated with pathophysiological differences and severity, to enhance the accuracy of prediction models and facilitate the selection of the optimal therapeutic approach. Future clinical trials should prioritize the inclusion of severe AIHA patients, particularly in the quest for rapidly acting novel agents.
Keywords: autoimmune hemolytic anemia; cold agglutinin disease; management; mortality; severe.
Copyright © 2023 Mulder, Evers, de Haas, Cruijsen, Bernelot Moens, Barcellini, Fattizzo and Vos.
Conflict of interest statement
MH and JV were employed by Sanquin Diagnostic Services. MH discloses consultancy for Johnson and Johnson and Omnia education. WB discloses consultancy and advisory board involvement with Agios, Alexion, Incyte, Novartis, and Sanofi, as well as research support provided by Alexion. BF declares receiving consultancy honoraria from Alexion and Janssen, as well as participating in the speakers' bureau for Alexion and Sobi. JV has declared receiving consultancy and advisory board honoraria from Sanofi and Janssen, research support from Beigene and Abbvie/Genmab, and participating in the speakers' bureau for BMS, Sanofi, and Amgen. All honoraria received are directed to the institute. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures