

Longitudinal Follow-Up of Children With HLHS and Association Between Norwood Shunt Type and Long-Term Outcomes: The SVR III Study
- PMID: 37795623
- PMCID: PMC10589429
- DOI: 10.1161/CIRCULATIONAHA.123.065192
Longitudinal Follow-Up of Children With HLHS and Association Between Norwood Shunt Type and Long-Term Outcomes: The SVR III Study
Abstract
Objective: In the SVR trial (Single Ventricle Reconstruction), newborns with hypoplastic left heart syndrome were randomly assigned to receive a modified Blalock-Taussig-Thomas shunt (mBTTS) or a right ventricle-to-pulmonary artery shunt (RVPAS) at Norwood operation. Transplant-free survival was superior in the RVPAS group at 1 year, but no longer differed by treatment group at 6 years; both treatment groups had accumulated important morbidities. In the third follow-up of this cohort (SVRIII [Long-Term Outcomes of Children With Hypoplastic Left Heart Syndrome and the Impact of Norwood Shunt Type]), we measured longitudinal outcomes and their risk factors through 12 years of age.
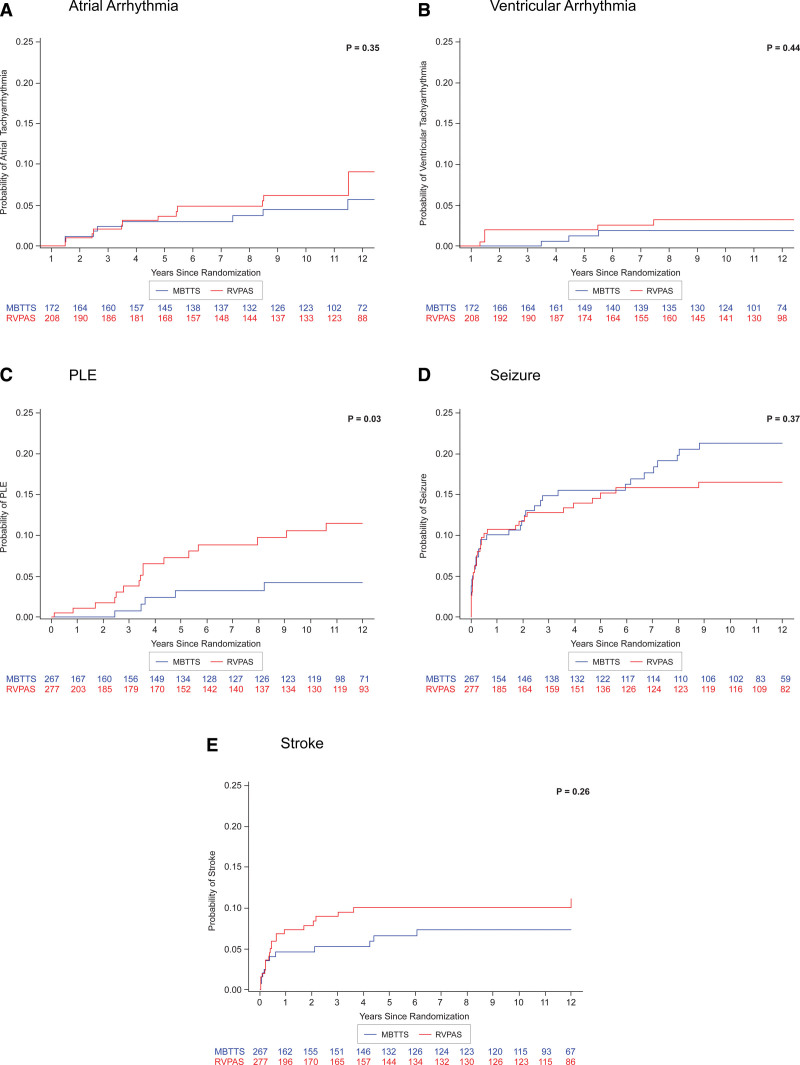
Methods: Annual medical history was collected through record review and telephone interviews. Cardiac magnetic resonance imaging (CMR), echocardiogram, and cycle ergometry cardiopulmonary exercise tests were performed at 10 through 14 years of age among participants with Fontan physiology. Differences in transplant-free survival and complication rates (eg, arrhythmias or protein-losing enteropathy) were identified through 12 years of age. The primary study outcome was right ventricular ejection fraction (RVEF) by CMR, and primary analyses were according to shunt type received. Multivariable linear and Cox regression models were created for RVEF by CMR and post-Fontan transplant-free survival.
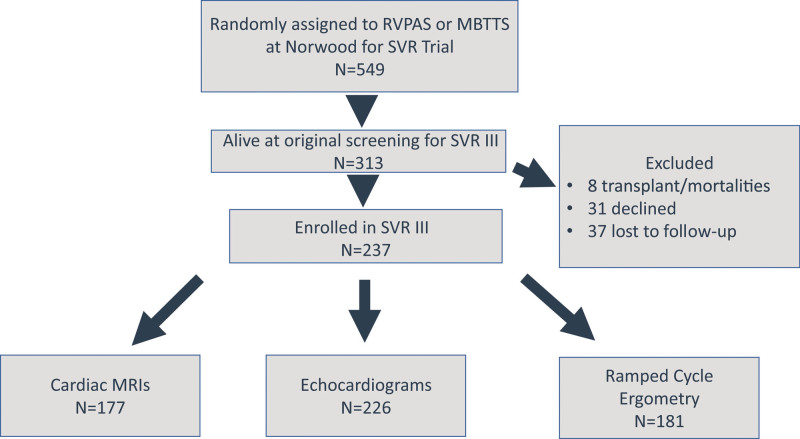
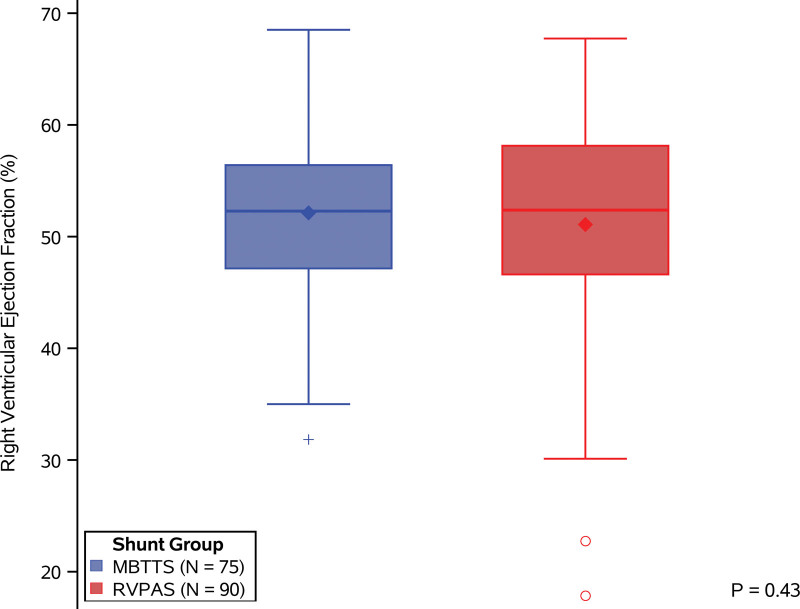
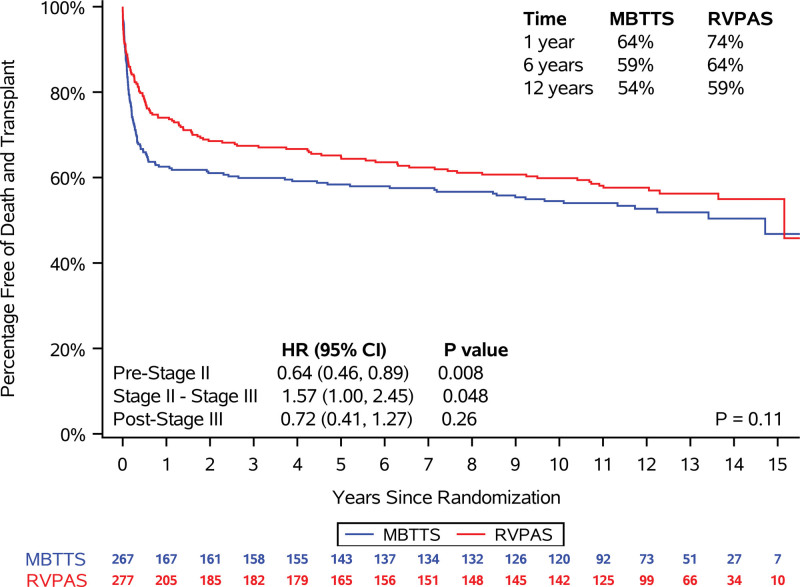
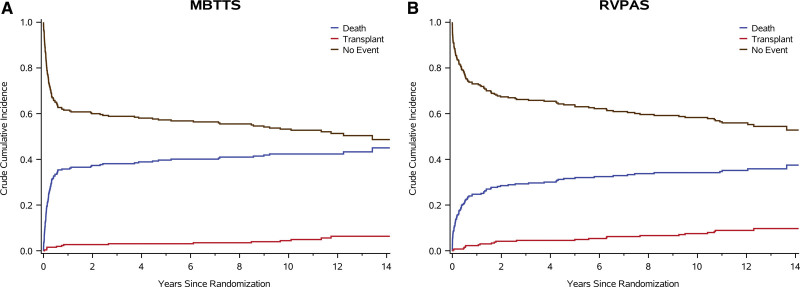
Results: Among 549 participants enrolled in SVR, 237 of 313 (76%; 60.7% male) transplant-free survivors (mBTTS, 105 of 147; RVPAS, 129 of 161; both, 3 of 5) participated in SVRIII. RVEF by CMR was similar in the shunt groups (RVPAS, 51±9.6 [n=90], and mBTTS, 52±7.4 [n=75]; P=0.43). The RVPAS and mBTTS groups did not differ in transplant-free survival by 12 years of age (163 of 277 [59%] versus 144 of 267 [54%], respectively; P=0.11), percentage predicted peak Vo2 for age and sex (74±18% [n=91] versus 72±18% [n=84]; P=0.71), or percentage predicted work rate for size and sex (65±20% versus 64±19%; P=0.65). The RVPAS versus mBTTS group had a higher cumulative incidence of protein-losing enteropathy (5% versus 2%; P=0.04) and of catheter interventions (14 versus 10 per 100 patient-years; P=0.01), but had similar rates of other complications.
Conclusions: By 12 years after the Norwood operation, shunt type has minimal association with RVEF, peak Vo2, complication rates, and transplant-free survival. RVEF is preserved among the subgroup of survivors who underwent CMR assessment. Low transplant-free survival, poor exercise performance, and accruing morbidities highlight the need for innovative strategies to improve long-term outcomes in patients with hypoplastic left heart syndrome.
Registration: URL: https://www.
Clinicaltrials: gov; Unique identifier: NCT0245531.
Keywords: hypoplastic left heart syndrome; longitudinal outcomes; single ventricle reconstruction.
Conflict of interest statement
Figures
References
-
- Norwood WI, Kirklin JK, Sanders SP. Hypoplastic left heart syndrome: experience with palliative surgery. Am J Cardiol. 1980;45:87–91. doi: 10.1016/0002-9149(80)90224-6 - PubMed
-
- Sano S, Ishino K, Kawada M, Honjo O. Right ventricle-pulmonary artery shunt in first-stage palliation of hypoplastic left heart syndrome. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2004;7:22–31. doi: 10.1053/j.pcsu.2004.02.023 - PubMed
-
- Ohye RG, Gaynor JW, Ghanayem NS, Goldberg CS, Laussen PC, Frommelt PC, Newburger JW, Pearson GD, Tabbutt S, Wernovsky G, et al. ; Pediatric Heart Network Investigators. Design and rationale of a randomized trial comparing the Blalock-Taussig and right ventricle-pulmonary artery shunts in the Norwood procedure. J Thorac Cardiovasc Surg. 2008;136:968–975. doi: 10.1016/j.jtcvs.2008.01.013 - PMC - PubMed
-
- Ohye RG, Sleeper LA, Mahony L, Newburger JW, Pearson GD, Lu M, Goldberg CS, Tabbutt S, Frommelt PC, Ghanayem NS, et al. ; Pediatric Heart Network Investigators. Comparison of shunt types in the Norwood procedure for single-ventricle lesions. N Engl J Med. 2010;362:1980–1992. doi: 10.1056/NEJMoa0912461 - PMC - PubMed
-
- Newburger JW, Sleeper LA, Gaynor JW, Hollenbeck-Pringle D, Frommelt PC, Li JS, Mahle WT, Williams IA, Atz AM, Burns KM, et al. ; Pediatric Heart Network Investigators. Transplant-free survival and interventions at 6 years in the SVR trial. Circulation. 2018;137:2246–2253. doi: 10.1161/CIRCULATIONAHA.117.029375 - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
