

Association of Preoperative Lung Function with Complications after Lobectomy Using Race-Neutral and Race-Specific Normative Equations
- PMID: 37796618
- PMCID: PMC10867917
- DOI: 10.1513/AnnalsATS.202305-396OC
Association of Preoperative Lung Function with Complications after Lobectomy Using Race-Neutral and Race-Specific Normative Equations
Abstract
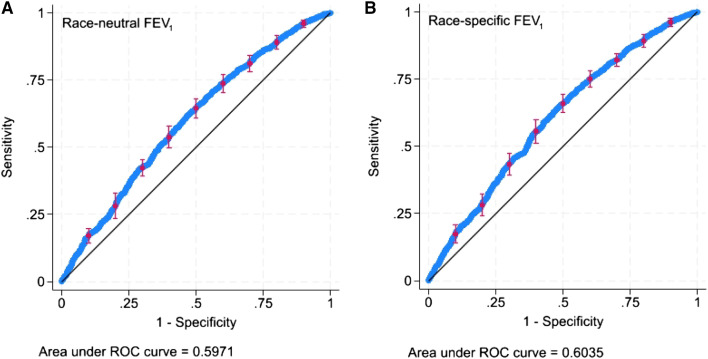
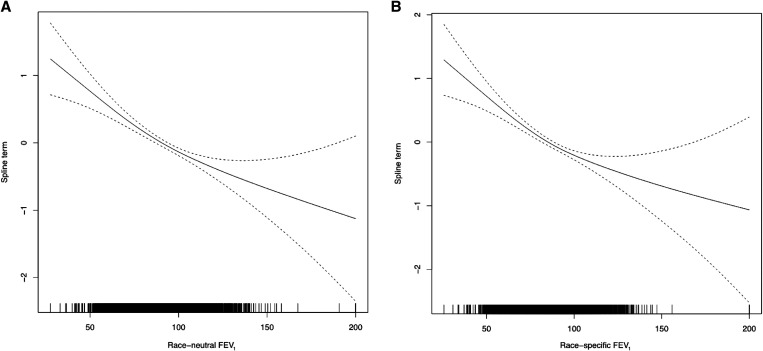
Rationale: Pulmonary function testing (PFT) is performed to aid patient selection before surgical resection for non-small cell lung cancer (NSCLC). The interpretation of PFT data relies on normative equations, which vary by race, but the relative strength of association of lung function using race-specific or race-neutral normative equations with postoperative pulmonary complications is unknown. Objectives: To compare the strength of association of lung function, using race-neutral or race-specific equations, with surgical complications after lobectomy for NSCLC. Methods: We studied 3,311 patients who underwent lobectomy for NSCLC and underwent preoperative PFT from 2001 to 2021. We used Global Lung Function Initiative equations to generate race-specific and race-neutral normative equations to calculate percentage predicted forced expiratory volume in 1 second (FEV1%). The primary outcome of interest was the occurrence of postoperative pulmonary complications within 30 days of surgery. We used unadjusted and race-adjusted logistic regression models and least absolute shrinkage and selection operator analyses adjusted for relevant comorbidities to measure the association of race-specific and race-neutral FEV1% with pulmonary complications. Results: Thirty-one percent of patients who underwent surgery experienced pulmonary complications. Higher FEV1, whether measured with race-neutral (odds ratio [OR], 0.98 per 1% change in FEV1% [95% confidence interval (CI), 0.98-0.99]; P < 0.001) or race-specific (OR, 0.98 per 1% change in FEV1% [95% CI, 0.98-0.98]; P < 0.001) normative equations, was associated with fewer postoperative pulmonary complications. The area under the receiver operator curve for pulmonary complications was similar for race-adjusted race-neutral (0.60) and race-specific (0.60) models. Using least absolute shrinkage and selection operator regression, higher FEV1% was similarly associated with a lower rate of pulmonary complications in race-neutral (OR, 0.99 per 1% [95% CI, 0.98-0.99]) and race-specific (OR, 0.99 per 1%; 95% CI, 0.98-0.99) models. The marginal effect of race on pulmonary complications was attenuated in all race-specific models compared with all race-neutral models. Conclusions: The choice of race-specific or race-neutral normative PFT equations does not meaningfully affect the association of lung function with pulmonary complications after lobectomy for NSCLC, but the use of race-neutral equations unmasks additional effects of self-identified race on pulmonary complications.
Keywords: lobectomy; non–small cell lung cancer; pulmonary complications; pulmonary function testing; race-based interpretation.
Figures
Comment in
-
Evaluating the Impact of Race-Neutral Interpretation of Preoperative Pulmonary Function.Ann Am Thorac Soc. 2024 Jan;21(1):32-34. doi: 10.1513/AnnalsATS.202309-834ED. Ann Am Thorac Soc. 2024. PMID: 38156898 Free PMC article. No abstract available.
Similar articles
-
Clinical Implications of Removing Race-Corrected Pulmonary Function Tests for African American Patients Requiring Surgery for Lung Cancer.JAMA Surg. 2023 Oct 1;158(10):1061-1068. doi: 10.1001/jamasurg.2023.3239. JAMA Surg. 2023. PMID: 37585181 Free PMC article. Clinical Trial.
-
Marginal pulmonary function should not preclude lobectomy in selected patients with non-small cell lung cancer.J Thorac Cardiovasc Surg. 2014 Feb;147(2):738-44; Discussion 744-6. doi: 10.1016/j.jtcvs.2013.09.064. Epub 2013 Nov 16. J Thorac Cardiovasc Surg. 2014. PMID: 24252944
-
Lobectomy improves ventilatory function in selected patients with severe COPD.Ann Thorac Surg. 1998 Sep;66(3):898-902. doi: 10.1016/s0003-4975(98)00697-3. Ann Thorac Surg. 1998. PMID: 9768948
-
Outcomes of lobectomy on pulmonary function for early stage non-small cell lung cancer (NSCLC) patients with chronic obstructive pulmonary disease (COPD).Thorac Cancer. 2020 Jul;11(7):1784-1789. doi: 10.1111/1759-7714.13445. Epub 2020 May 6. Thorac Cancer. 2020. PMID: 32374491 Free PMC article. Review.
-
Systematic review and meta‑analysis of factors predicting postoperative lung function after lung cancer resection.Wideochir Inne Tech Maloinwazyjne. 2024 Jul 31;19(3):289-298. doi: 10.20452/wiitm.2024.17892. eCollection 2024 Oct 16. Wideochir Inne Tech Maloinwazyjne. 2024. PMID: 40041108 Free PMC article.
Cited by
-
Lung Function Trajectory Using Race-Specific vs Race-Neutral Global Lung Function Initiative Coefficients.JAMA Netw Open. 2025 Apr 1;8(4):e257304. doi: 10.1001/jamanetworkopen.2025.7304. JAMA Netw Open. 2025. PMID: 40279124 Free PMC article.
-
Evaluating the Impact of Race-Neutral Interpretation of Preoperative Pulmonary Function.Ann Am Thorac Soc. 2024 Jan;21(1):32-34. doi: 10.1513/AnnalsATS.202309-834ED. Ann Am Thorac Soc. 2024. PMID: 38156898 Free PMC article. No abstract available.
-
Framing the Consequences of Implementing Race-Neutral Interpretation of Spirometry.Ann Am Thorac Soc. 2024 Sep;21(9):1249-1250. doi: 10.1513/AnnalsATS.202407-676ED. Ann Am Thorac Soc. 2024. PMID: 39212421 Free PMC article. No abstract available.
References
-
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin . 2023;73:17–48. - PubMed
-
- Keagy BA, Lores ME, Starek PJ, Murray GF, Lucas CL, Wilcox BR. Elective pulmonary lobectomy: factors associated with morbidity and operative mortality. Ann Thorac Surg . 1985;40:349–352. - PubMed
-
- Varela G, Brunelli A, Rocco G, Novoa N, Refai M, Jiménez MF, et al. Measured FEV1 in the first postoperative day, and not ppoFEV1, is the best predictor of cardio-respiratory morbidity after lung resection. Eur J Cardiothorac Surg . 2007;31:518–521. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
