

An "off-the-shelf" CD2 universal CAR-T therapy for T-cell malignancies
- PMID: 37798328
- PMCID: PMC10681896
- DOI: 10.1038/s41375-023-02039-z
An "off-the-shelf" CD2 universal CAR-T therapy for T-cell malignancies
Abstract
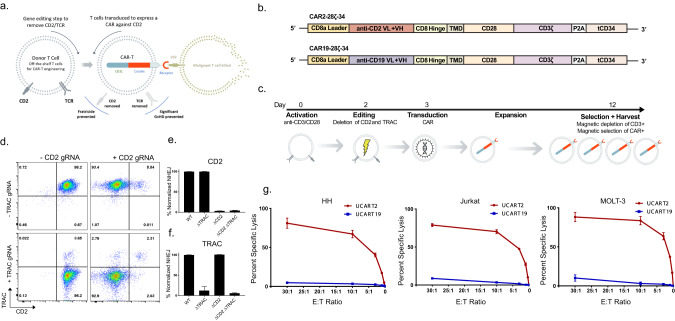
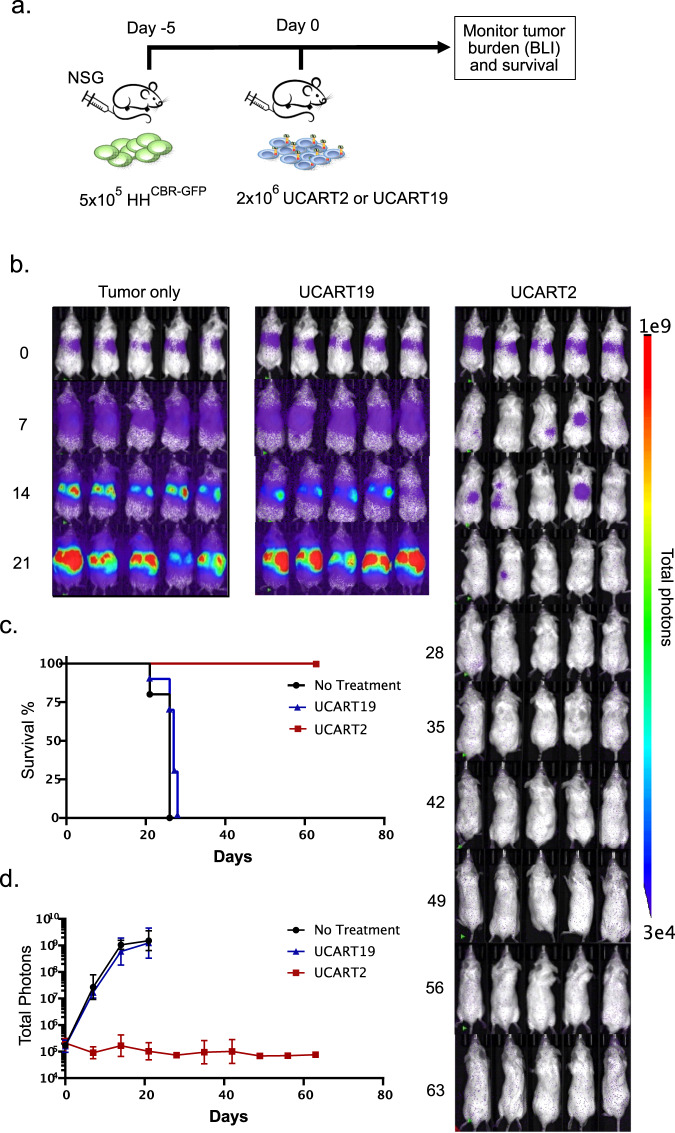
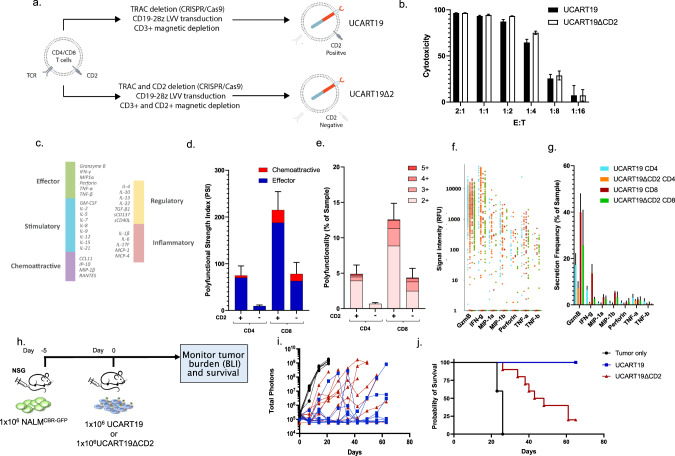
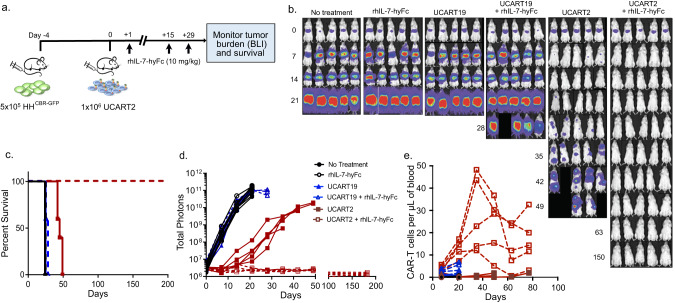
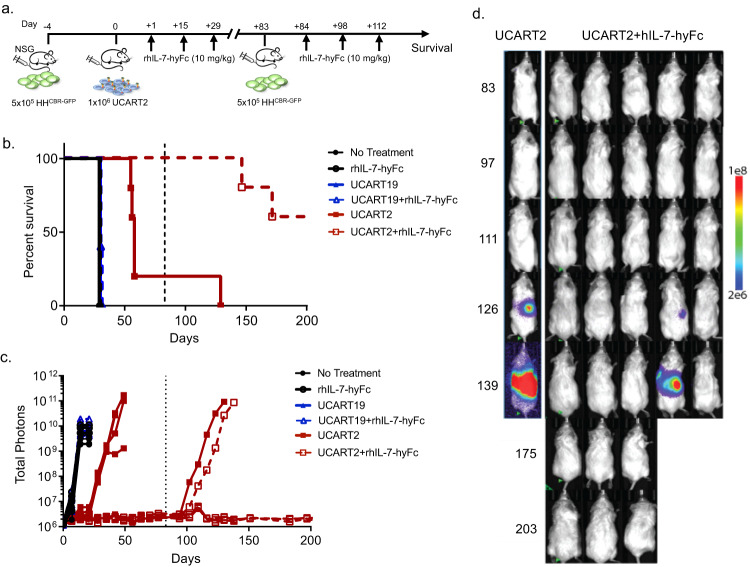
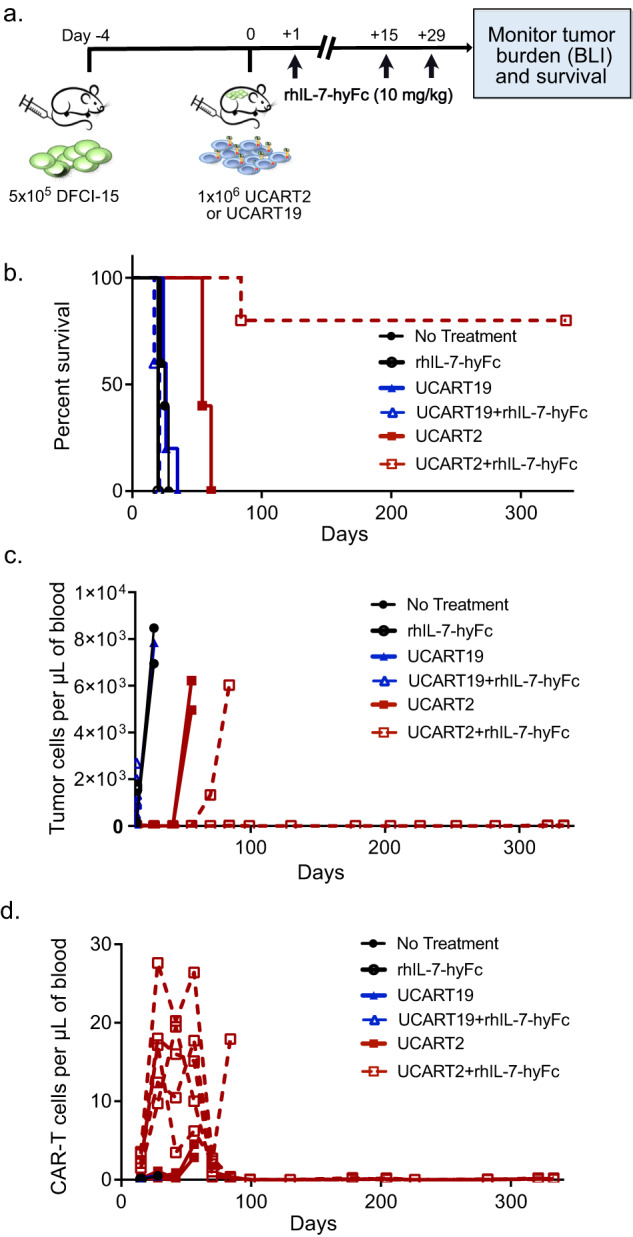
T-cell malignancies are associated with frequent relapse and high morbidity, which is partly due to the lack of effective or targeted treatment options. To broaden the use of CAR-T cells in pan T-cell malignancies, we developed an allogeneic "universal" CD2-targeting CAR-T cell (UCART2), in which the CD2 antigen is deleted to prevent fratricide, and the T-cell receptor is removed to prevent GvHD. UCART2 demonstrated efficacy against T-ALL and CTCL and prolonged the survival of tumor-engrafted NSG mice in vivo. To evaluate the impact of CD2 on CAR-T function, we generated CD19 CAR-T cells (UCART19) with or without CD2 deletion, single-cell secretome analysis revealed that CD2 deletion in UCART19 reduced frequencies of the effector cytokines (Granzyme-B and IFN-γ). We also observed that UCART19ΔCD2 had reduced anti-tumor efficacy compared to UCART19 in a CD19+NALM6 xenograft model. Of note is that the reduced efficacy resulting from CD2 deletion was reversed when combined with rhIL-7-hyFc, a long-acting recombinant human interleukin-7. Treatment with rhIL-7-hyFc prolonged UCART2 persistence and increased survival in both the tumor re-challenge model and primary patient T-ALL model in vivo. Together, these data suggest that allogeneic fratricide-resistant UCART2, in combination with rhIL-7-hyFc, could be a suitable approach for treating T-cell malignancies.
© 2023. The Author(s).
Conflict of interest statement
MYK, KWS, JO, MLC, and JFD are creators/inventors of a patent on the use of IL-7 to enhance CAR T cell function. MLC is currently employed by and has equity ownership in Wugen. JFD receives research funding from Amphivena Therapeutics, NeoImmuneTech, Macrogenics, Incyte, Bioline Rx, Wugen; has equity ownership in Magenta Therapeutics, Wugen; consults for Incyte, RiverVest Venture Partners, hC Bioscience, Inc.; and is a board member for RiverVest Venture Partners, Magenta Therapeutics. AJC is currently employed by BlueSphere Bio and has equity ownership in Wugen. GR and RT are currently employed by Integrated DNA Technologies. BHL is currently employed by NeoImmuneTech, Inc. The remaining authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
