

Precision subclassification of type 2 diabetes: a systematic review
- PMID: 37798471
- PMCID: PMC10556101
- DOI: 10.1038/s43856-023-00360-3
Precision subclassification of type 2 diabetes: a systematic review
Abstract
Background: Heterogeneity in type 2 diabetes presentation and progression suggests that precision medicine interventions could improve clinical outcomes. We undertook a systematic review to determine whether strategies to subclassify type 2 diabetes were associated with high quality evidence, reproducible results and improved outcomes for patients.
Methods: We searched PubMed and Embase for publications that used 'simple subclassification' approaches using simple categorisation of clinical characteristics, or 'complex subclassification' approaches which used machine learning or 'omics approaches in people with established type 2 diabetes. We excluded other diabetes subtypes and those predicting incident type 2 diabetes. We assessed quality, reproducibility and clinical relevance of extracted full-text articles and qualitatively synthesised a summary of subclassification approaches.
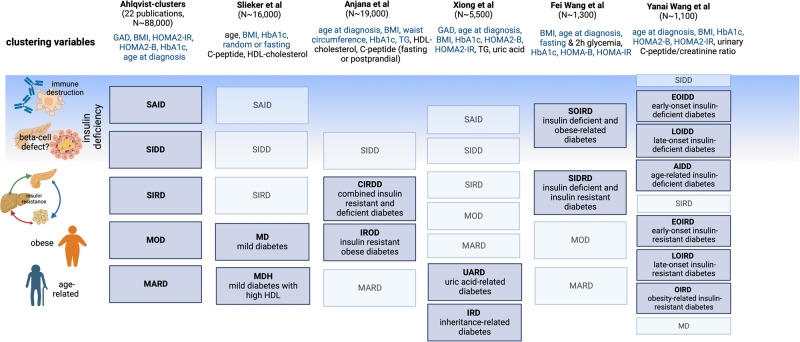
Results: Here we show data from 51 studies that demonstrate many simple stratification approaches, but none have been replicated and many are not associated with meaningful clinical outcomes. Complex stratification was reviewed in 62 studies and produced reproducible subtypes of type 2 diabetes that are associated with outcomes. Both approaches require a higher grade of evidence but support the premise that type 2 diabetes can be subclassified into clinically meaningful subtypes.
Conclusion: Critical next steps toward clinical implementation are to test whether subtypes exist in more diverse ancestries and whether tailoring interventions to subtypes will improve outcomes.
Plain language summary
In people with type 2 diabetes there may be differences in the way people present, including for example, their symptoms, body weight or how much insulin they make. We looked at recent publications describing research in this area to see whether it is possible to separate people with type 2 diabetes into different subgroups and, if so, whether these groupings were useful for patients. We found that it is possible to group people with type 2 diabetes into different subgroups and being in one subgroup can be more strongly linked to the likelihood of developing complications over others. This might mean that in the future we can treat people in different subgroups differently in ways that improves their treatment and their health but it requires further study.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare the following conflicts of interest. S.M. has investigator-initiated funding from DexCom, has received speaker fees (donated to institution) from Sanofi for a scientific talk over which she had full control of content and serves on the Board of Trustees for the Diabetes Research & Wellness Foundation (UK); R.W. declares lecture fees from Novo Nordisk, Sanofi and Eli Lilly. He served on an advisory board for Akcea Therapeutics, Daiichi Sankyo, Sanofi, Eli Lilly, and NovoNordisk; S.J.C. reports a close family member employed by a Johnson & Johnson company; R.H.S. reports fees from Novo Nordisk and Amgen; L.K.B. has received consulting honoraria from Bayer, Novo Nordisk, Sanofi, Lilly, and Xeris; W.H.H.S. reported as Advisor and/or Speaker for AstraZeneca, Bayer HealthCare, Boehringer Ingelheim Pharmaceuticals., Daiichi-Sankyo, Eli Lilly and Company, Merck Sharp & Dohme, Mitsubishi Tanabe Pharma Corporation, Novartis Pharmaceuticals, Novo Nordisk, Pfizer, Sanofi-Aventis, Takeda Pharmaceutical Company; N.S. is Senior Associate Editor of Diabetes and has received speaking honoraria from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novartis, Novo Nordisk, Pfizer and Sanofi for scientific talks over which he had full control of content; M.G. has served on an advisory board for Nestle Health Science; E.S. is a Deputy Editor of Diabetes Care and a member of the editorial board of Diabetologia and receives payments from Wolters Kluwer for chapters and laboratory monographs in UpToDate on measurements of glycemic control and screening tests for type 2 diabetes; J.C.F. has received speaking honoraria from AstraZeneca and Novo Nordisk for scientific talks over which he had full control of content; J.B.M. is an Academic Associate for Quest Inc. Diagnostics R&D; M.U. reports an unpaid collaborator with AstraZeneca. All other authors have no disclosures. A.L. reports a close family member employed by Merck & Co., Inc.
Figures


Update of
-
Systematic review of precision subclassification of type 2 diabetes.medRxiv [Preprint]. 2023 Apr 20:2023.04.19.23288577. doi: 10.1101/2023.04.19.23288577. medRxiv. 2023. Update in: Commun Med (Lond). 2023 Oct 5;3(1):138. doi: 10.1038/s43856-023-00360-3. PMID: 37131632 Free PMC article. Updated. Preprint.
References
-
- Diabetes Atlas 10th Edition, World Health Organisation. https://diabetesatlas.org/atlas/tenth-edition/, accessed 6 Jun 2023 (2021).
-
- Prando R, et al. Is type 2 diabetes a different disease in obese and nonobese patients? Diabetes Care. 1998;21:1680–1685. - PubMed
Grants and funding
- R21 DK125888/DK/NIDDK NIH HHS/United States
- T32 DK007028/DK/NIDDK NIH HHS/United States
- K24 HL152440/HL/NHLBI NIH HHS/United States
- K23 DK133690/DK/NIDDK NIH HHS/United States
- K23 DK114551/DK/NIDDK NIH HHS/United States
- T32 HL007024/HL/NHLBI NIH HHS/United States
- P30 DK063491/DK/NIDDK NIH HHS/United States
- U01 DK078616/DK/NIDDK NIH HHS/United States
- RG/17/12/33167/BHF_/British Heart Foundation/United Kingdom
- K24 HL157960/HL/NHLBI NIH HHS/United States
- 210752/Z/18/Z/WT_/Wellcome Trust/United Kingdom
- MC_UU_00014/4/MRC_/Medical Research Council/United Kingdom
- R01 HL151855/HL/NHLBI NIH HHS/United States
- UM1 DK078616/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
