

Critical care capacity and care bundles on medical wards in Malawi: a cross-sectional study
- PMID: 37798681
- PMCID: PMC10557270
- DOI: 10.1186/s12913-023-10014-8
Critical care capacity and care bundles on medical wards in Malawi: a cross-sectional study
Abstract
Introduction: As low-income countries (LICs) shoulder a disproportionate share of the world's burden of critical illnesses, they must continue to build critical care capacity outside conventional intensive care units (ICUs) to address mortality and morbidity, including on general medical wards. A lack of data on the ability to treat critical illness, especially in non-ICU settings in LICs, hinders efforts to improve outcomes.
Methods: This was a secondary analysis of the cross-sectional Malawi Emergency and Critical Care (MECC) survey, administered from January to February 2020, to a random sample of nine public sector district hospitals and all four central hospitals in Malawi. This analysis describes inputs, systems, and barriers to care in district hospitals compared to central hospital medical wards, including if any medical wards fit the World Federation of Intensive and Critical Care Medicine (WFSICCM) definition of a level 1 ICU. We grouped items into essential care bundles for service readiness compared using Fisher's exact test.
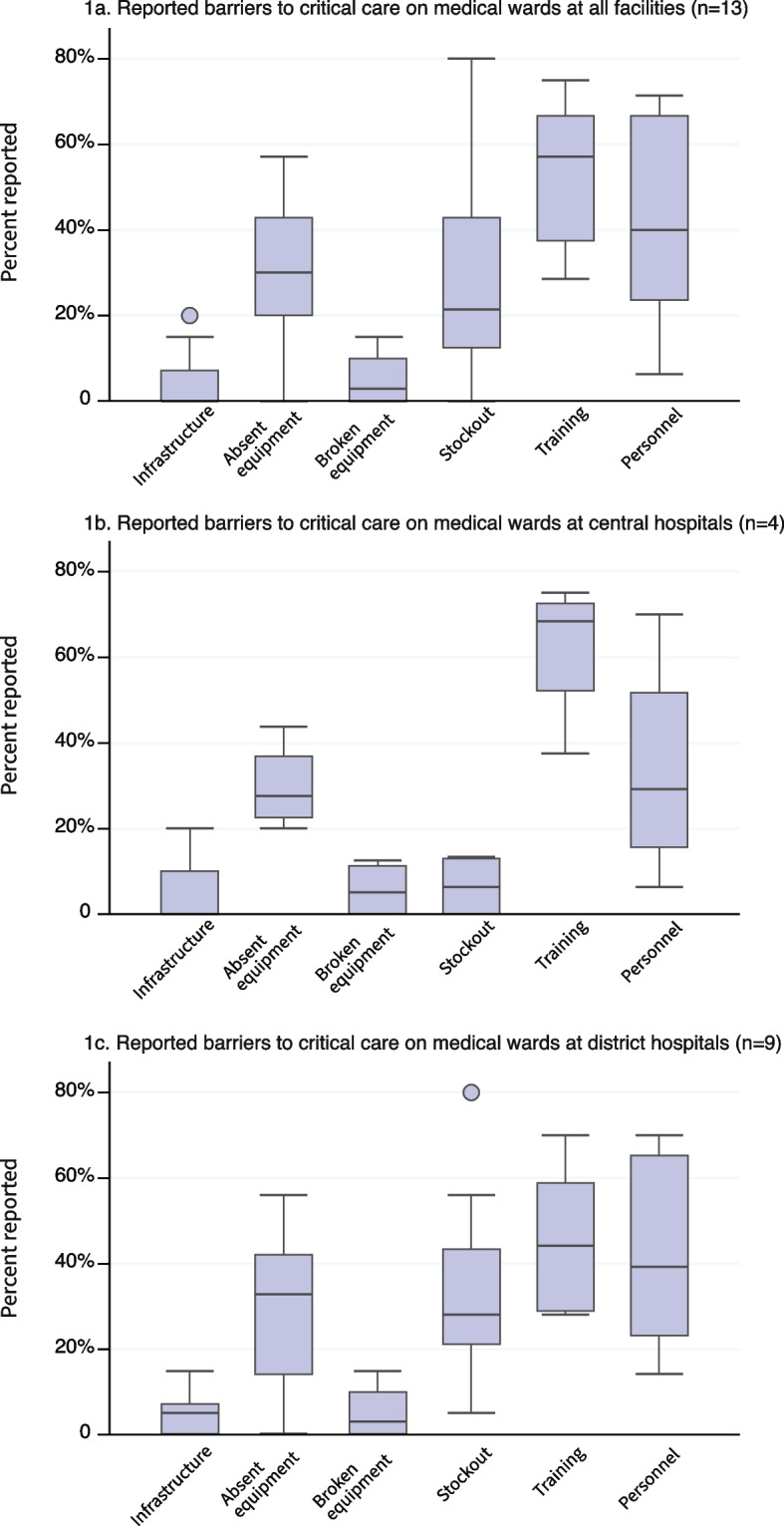
Results: From the 13 hospitals, we analysed data from 39 medical ward staff members through staffing, infrastructure, equipment, and systems domains. No medical wards met the WFSICCM definition of level 1 ICU. The most common barriers in district hospital medical wards compared to central hospital wards were stock-outs (29%, Cl: 21% to 44% vs 6%, Cl: 0% to 13%) and personnel shortages (40%, Cl: 24% to 67% vs 29%, Cl: 16% to 52%) but central hospital wards reported a higher proportion of training barriers (68%, Cl: 52% to 73% vs 45%, Cl: 29% to 60%). No differences were statistically significant.
Conclusion: Despite current gaps in resources to consistently care for critically ill patients in medical wards, this study shows that with modest inputs, the provision of simple life-saving critical care is within reach. Required inputs for care provision can be informed from this study.
Keywords: Barriers; Care capacity; Critical care; Medical ward.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
PDS reports consulting fees from the University of California-San Francisco/Sustaining Technical and Analytic Resources and funding from Unitaid (Grant SPHQ15-LOA-045). JSM is the Chief Medical Officer at Partners In Health and sits on the boards of Village Health Works (Burundi/Muso and Mali), The Institute for Justice and Democracy in Haiti, and Free Speech for People. EC, NK, MN, RM, EBW, KS, AB, TM, MK, GB, and SAR have no competing interests.
Figures
References
-
- Baelani I, Jochberger S, Laimer T, Otieno D, Kabutu J, Wilson I, et al. Availability of critical care resources to treat patients with severe sepsis or septic shock in Africa: a self-reported, continent-wide survey of anaesthesia providers. Crit Care (London, England) 2011;15(1):R10. doi: 10.1186/cc9410. - DOI - PMC - PubMed
-
- GBD 2019 Diseases and Injuries Collaborators Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (London, England). 2020;396(10258):1204–22. doi: 10.1016/S0140-6736(20)30925-9. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
