

Tenosynovial giant cell tumor: a case report
- PMID: 37798760
- PMCID: PMC10557153
- DOI: 10.1186/s13256-023-04156-w
Tenosynovial giant cell tumor: a case report
Abstract
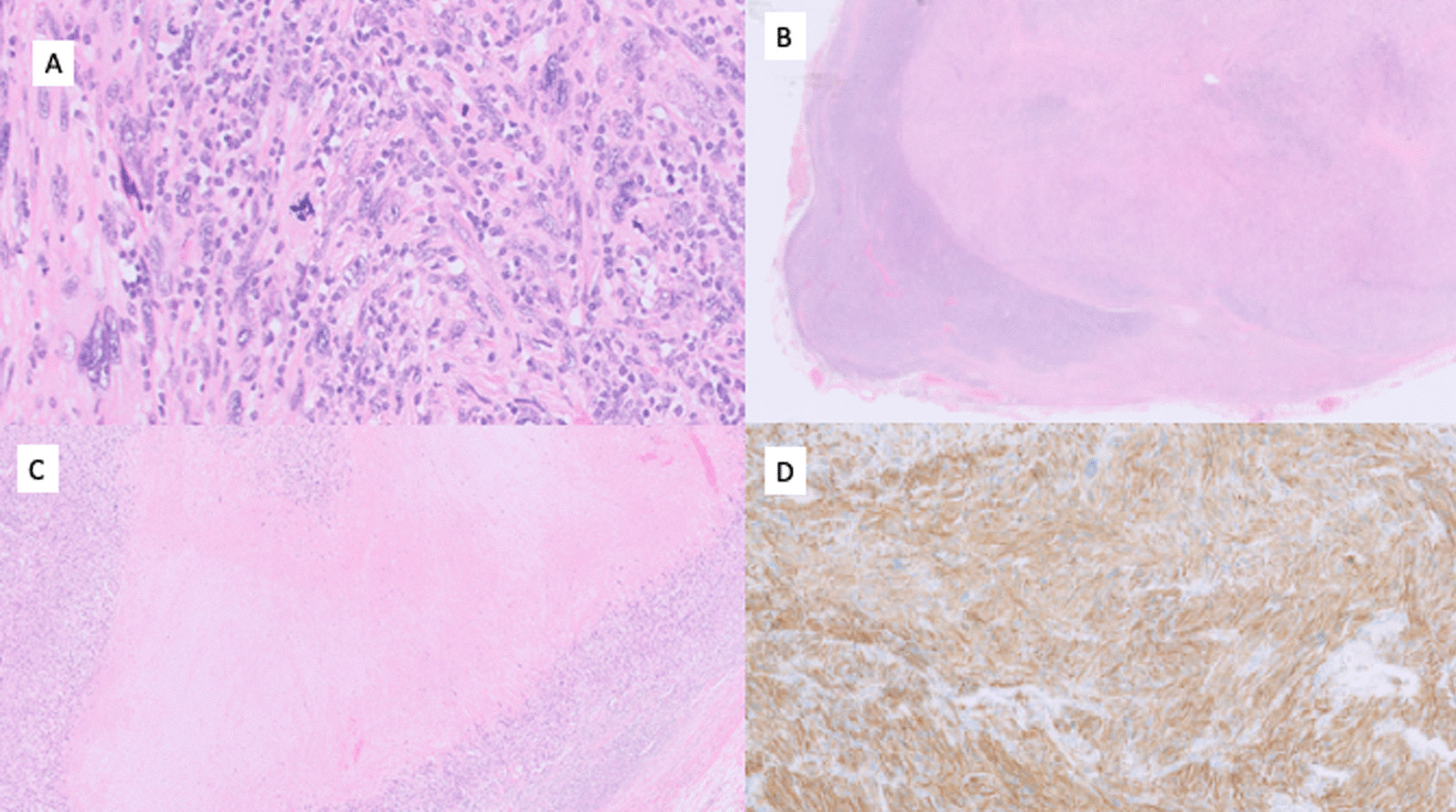
Background: This case reports the synchronous diagnosis of two rare unrelated diseases; leiomyosarcoma and tenosynovial giant cell tumor of the knee. It focuses on the challenges of diagnosing tenosynovial giant cell tumor, including cognitive biases in clinical medicine that delay diagnosis. It also demonstrates the pathogenic etiology of tenosynovial giant cell tumor, evidenced by the transient deterioration of the patients' knee symptoms following the administration of prophylactic granulocyte colony-stimulating factor given as part of the chemotherapeutic regime for leiomyosarcoma.
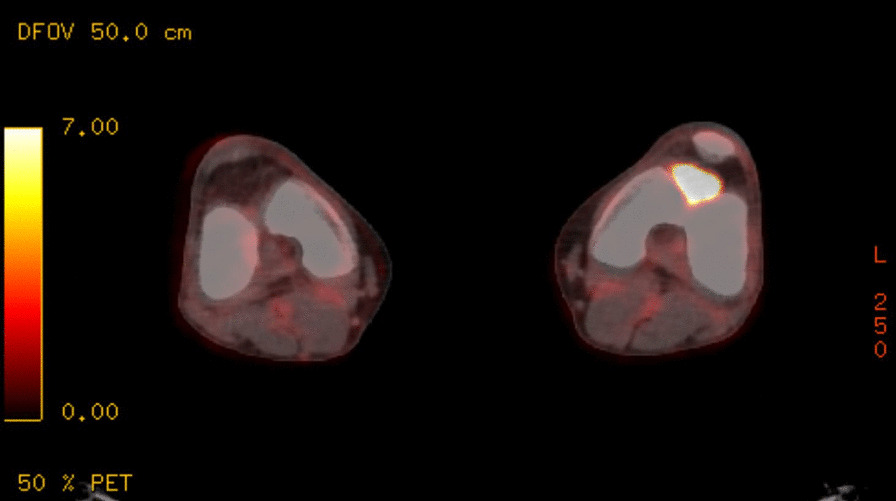
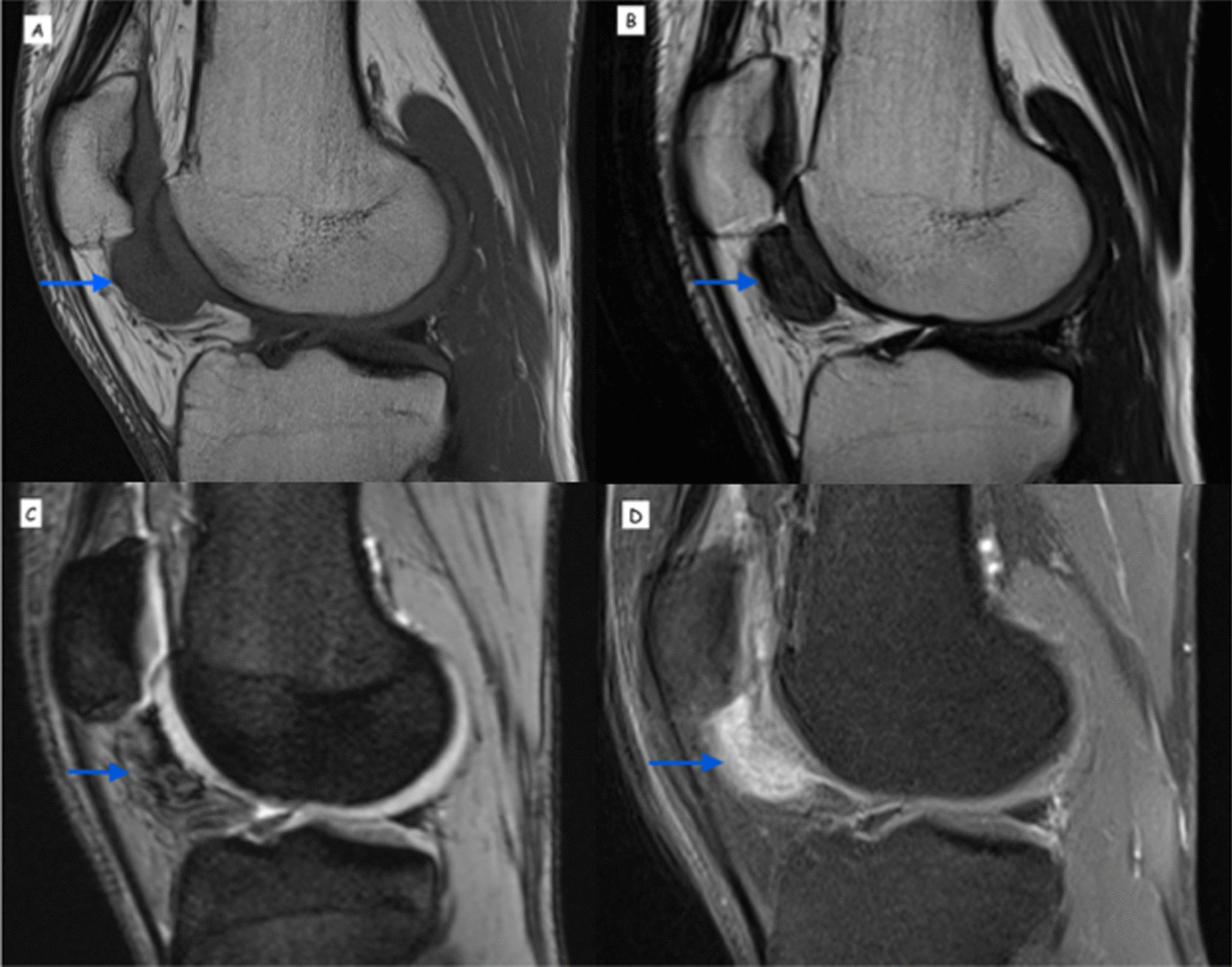
Case presentation: A 37-year-old Caucasian man presented with a left groin lump and left knee pain with swelling and locking. Investigations including positron emission tomography-computed tomography and biopsy revealed leiomyosarcoma in a lymph node likely related to the spermatic cord, with high-grade uptake in the left knee that was presumed to be the primary site. His knee symptoms temporarily worsened each time granulocyte colony-stimulating factor was administered with each cycle of chemotherapy for leiomyosarcoma to help combat myelosuppressive toxicity. Subsequent magnetic resonance imaging and biopsy of the knee confirmed a tenosynovial giant cell tumor. His knee symptoms relating to the tenosynovial giant cell tumor improved following the completion of his leiomyosarcoma treatment.
Conclusions: Tenosynovial giant cell tumor remains a diagnostic challenge. We discuss the key clinical features and investigations that aid prompt diagnosis. The National Comprehensive Cancer Network clinical practice guidelines for soft tissue sarcoma have recently been updated to include the pharmacological management of tenosynovial giant cell tumor. Our case discussion provides an up-to-date review of the evidence for optimal management of patients with tenosynovial giant cell tumor, with a particular focus on novel pharmacological options that exploit underlying pathogenesis.
Keywords: Joint tumors; Pigmented villonodular synovitis; Sarcoma; Tenosynovial giant cell tumor.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Organisation mondiale de la santé, Centre international de recherche sur le cancer (eds). Soft tissue and bone tumours. 5th ed. Geneva: OMS, 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
