

Assessment of anti-malondialdehyde-acetaldehyde antibody frequencies in rheumatoid arthritis with new data from two independent cohorts, meta-analysis, and meta-regression
- PMID: 37798800
- PMCID: PMC10552211
- DOI: 10.1186/s13075-023-03180-x
Assessment of anti-malondialdehyde-acetaldehyde antibody frequencies in rheumatoid arthritis with new data from two independent cohorts, meta-analysis, and meta-regression
Abstract
Background: Autoantibodies are critical elements in RA pathogenesis and clinical assessment. The anti-malondialdehyde-acetaldehyde (anti-MAA) antibodies are potentially useful because of their claimed high sensitivity for all RA patients, including those lacking RF and anti-CCP antibodies. Therefore, we aimed to replicate these findings.
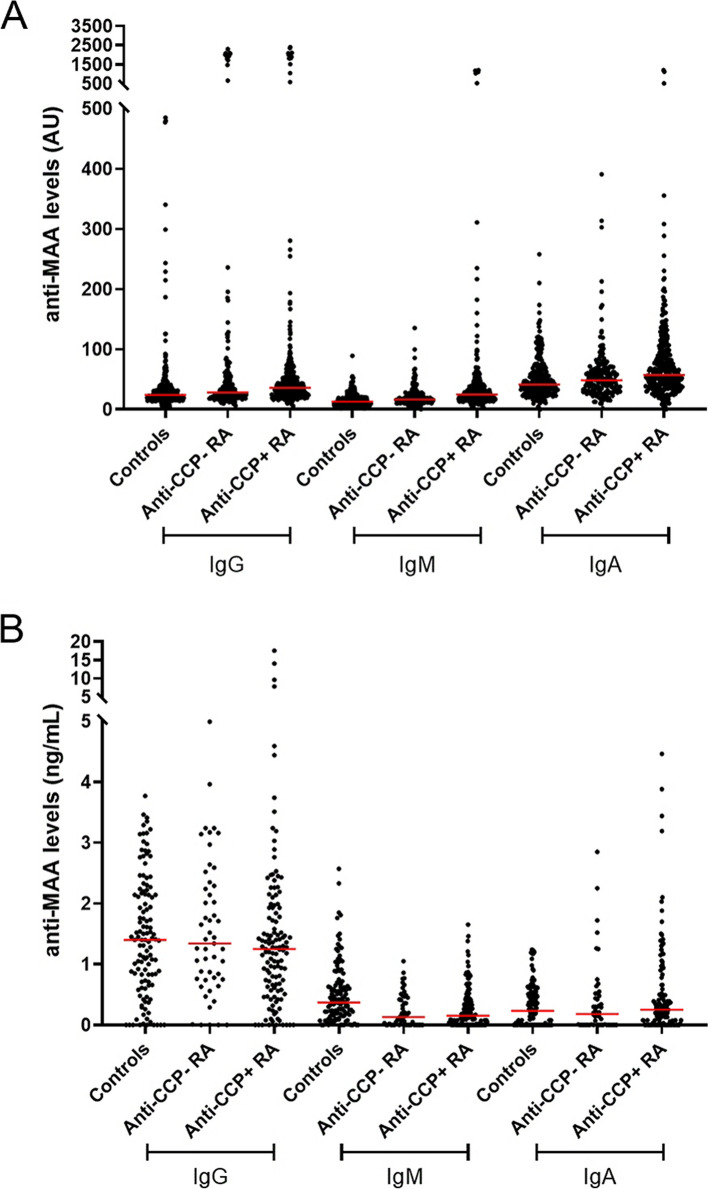
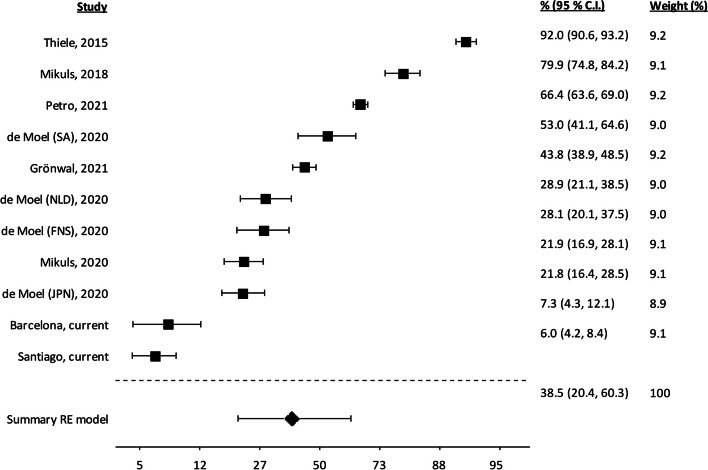
Methods: We independently attempted replication in Santiago and Barcelona using sera from 517 and 178 RA patients and 272 and 120 healthy controls, respectively. ELISA protocols for anti-MAA antibodies included five antigens (human serum albumin in three formulations, fibrinogen, and a synthetic peptide) and assays for the IgG, IgM, and IgA isotypes. We integrated our results with information found by searching the Web of Science for reports of anti-MAA antibodies in RA. The available patients (4989 in 11 sets) were included in a meta-analysis aimed at heterogeneity between studies. Factors accounting for heterogeneity were assessed with meta-regression.
Results: The sensitivity of anti-MAA antibodies in our RA patients was low, even in seropositive patients, with the percentage of positives below 23% for all ELISA conditions. Our results and bibliographic research showed IgG anti-MAA positive patients ranging from 6 to 92%. The extreme between-studies heterogeneity could be explained (up to 43%) in univariate analysis by sex, African ethnicity, the site of study, or recruitment from the military. The best model, including African ancestry and smoking, explained a high heterogeneity fraction (74%).
Conclusion: Anti-MAA antibody sensitivity is extremely variable between RA patient collections. A substantial fraction of this variability cannot be attributed to ELISA protocols. On the contrary, heterogeneity is determined by complex factors that include African ethnicity, smoking, and sex.
Keywords: Autoantibodies; Biomarker; Heterogeneity; Meta-analysis; Post-translational modifications; Rheumatoid arthritis.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Gravallese EM, Firestein GS. Rheumatoid arthritis - common origins, divergent mechanisms. N Engl J Med. 2023;388(6):529–542. - PubMed
-
- Smolen JS, Aletaha D, Barton A, Burmester GR, Emery P, Firestein GS, et al. Rheumatoid arthritis. Nat Rev Dis Primers. 2018;4:18001. - PubMed
-
- Darrah E, Andrade F. Editorial: citrullination, and carbamylation, and malondialdehyde-acetaldehyde! Oh my! Entering the forest of autoantigen modifications in rheumatoid arthritis. Arthritis Rheumatol. 2015;67(3):604–608. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
