

Concurrent Primary Hyperparathyroidism and Sarcoidosis in a Patient With Severe Hypercalcemia
- PMID: 37799241
- PMCID: PMC10550306
- DOI: 10.7759/cureus.44669
Concurrent Primary Hyperparathyroidism and Sarcoidosis in a Patient With Severe Hypercalcemia
Abstract
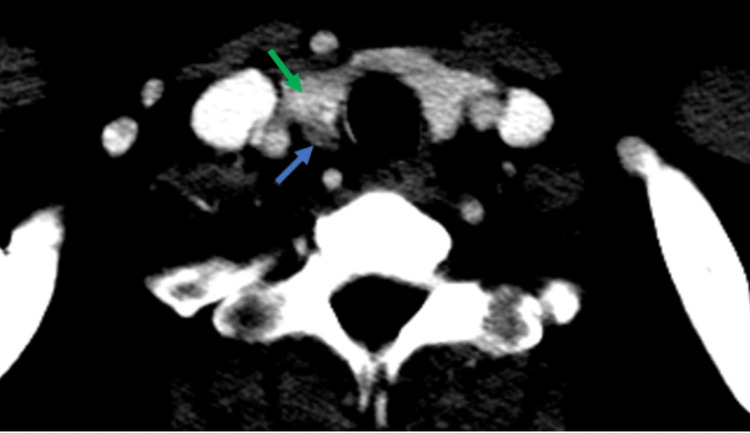
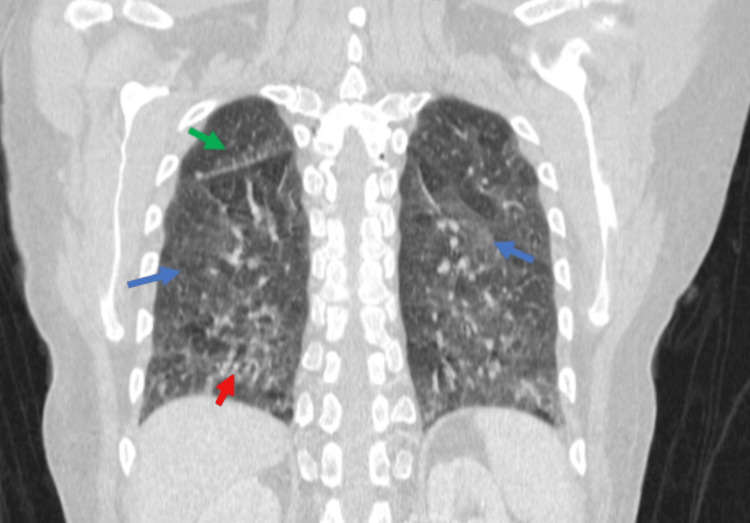
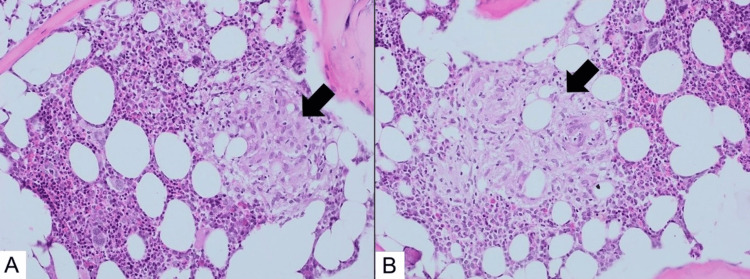
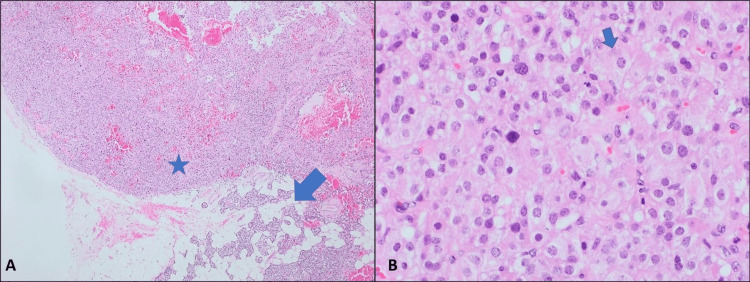
Hypercalcemia is a common biochemical abnormality caused by various etiologies, with primary hyperparathyroidism (PHPT) and malignancies being the most common culprits. Differentiating between PTH-dependent and PTH-independent hypercalcemia is crucial in clinical practice. However, in certain clinical contexts, it is important to consider the rare occurrence of two separate conditions causing hypercalcemia simultaneously. Herein, we have described the case of a patient who presented with high serum calcium, a normal PTH level, and histopathological evidence of active granulomatous disease, indicating the presence of both PHPT and sarcoidosis. The coexistence of these conditions poses diagnostic challenges due to their biochemical and clinical similarities. This case highlights the importance of individualized management for patients with concurrent conditions contributing to hypercalcemia. It also emphasizes the need for further research to unravel the underlying interactions between PHPT and sarcoidosis in the context of calcium metabolism. A better understanding of these interactions can guide optimal diagnostic and therapeutic strategies for patients with complex presentations of hypercalcemia.
Keywords: adult primary hyperparathyroidism; endocrinology; hypercalcemia; parathyroid gland adenoma; sarcoidosis.
Copyright © 2023, Ayyad et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Hypercalcemia: A Review.JAMA. 2022 Oct 25;328(16):1624-1636. doi: 10.1001/jama.2022.18331. JAMA. 2022. PMID: 36282253 Review.
-
Preoperative normal level of parathyroid hormone signifies an early and mild form of primary hyperparathyroidism.World J Surg. 2003 Apr;27(4):481-5. doi: 10.1007/s00268-002-6649-1. World J Surg. 2003. PMID: 12658497
-
Concomitant familial hypocalciuric hypercalcemia and single parathyroid adenoma: a case report.J Med Case Rep. 2021 Sep 24;15(1):471. doi: 10.1186/s13256-021-03051-6. J Med Case Rep. 2021. PMID: 34556169 Free PMC article.
-
A Therapeutic Approach to Primary Hyperparathyroidism: A Collaborative Evaluation Between Endocrinology and Surgery.Cureus. 2023 Jan 24;15(1):e34157. doi: 10.7759/cureus.34157. eCollection 2023 Jan. Cureus. 2023. PMID: 36843806 Free PMC article.
-
Association of primary hyperparathyroidism and humoral hypercalcemia of malignancy in a patient with clear cell renal carcinoma.Arch Endocrinol Metab. 2015 Feb;59(1):84-8. doi: 10.1590/2359-3997000000015. Arch Endocrinol Metab. 2015. PMID: 25926120 Review.
Cited by
-
Calcium Chaos in Sarcoidosis: A Tale of Severe Hypercalcemia's Diagnostic Challenge.Cureus. 2024 Mar 16;16(3):e56271. doi: 10.7759/cureus.56271. eCollection 2024 Mar. Cureus. 2024. PMID: 38623131 Free PMC article.
References
-
- The diagnosis and management of hypercalcaemia. Minisola S, Pepe J, Piemonte S, Cipriani C. BMJ. 2015;350:0. - PubMed
-
- Calcium metabolism in sarcoidosis and its clinical implications. Conron M, Young C, Beynon HL. Rheumatology (Oxford) 2000;39:707–713. - PubMed
-
- Hypercalcemia in sarcoidosis [Article in Japanese] Katakami N. https://pubmed.ncbi.nlm.nih.gov/12233075/ Nihon Rinsho. 2002;60:1778–1784. - PubMed
-
- Endocrine complications of sarcoidosis. Bell NH. Endocrinol Metab Clin North Am. 1991;20:645–654. - PubMed
-
- Parathyroid hormone and its related peptides in bone metabolism. Chen T, Wang Y, Hao Z, Hu Y, Li J. Biochem Pharmacol. 2021;192:114669. - PubMed
Publication types
LinkOut - more resources
Full Text Sources