

Epidemiology, natural evolution, pathogenesis, clinical spectrum, and management of Legg-Calvé-Perthes
- PMID: 37799310
- PMCID: PMC10549695
- DOI: 10.1177/18632521231203009
Epidemiology, natural evolution, pathogenesis, clinical spectrum, and management of Legg-Calvé-Perthes
Abstract
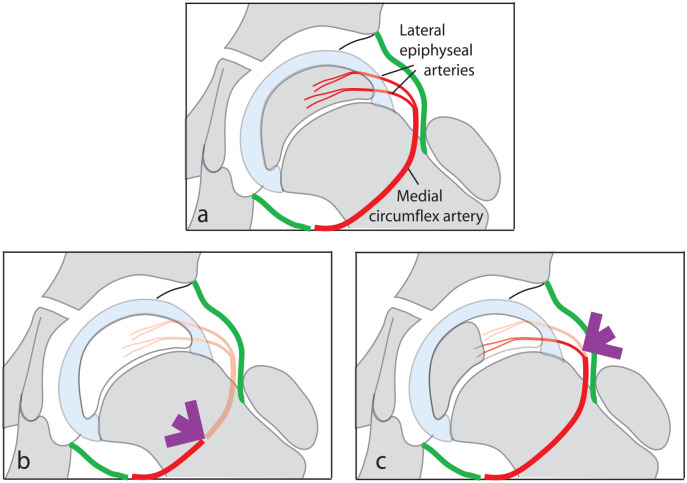
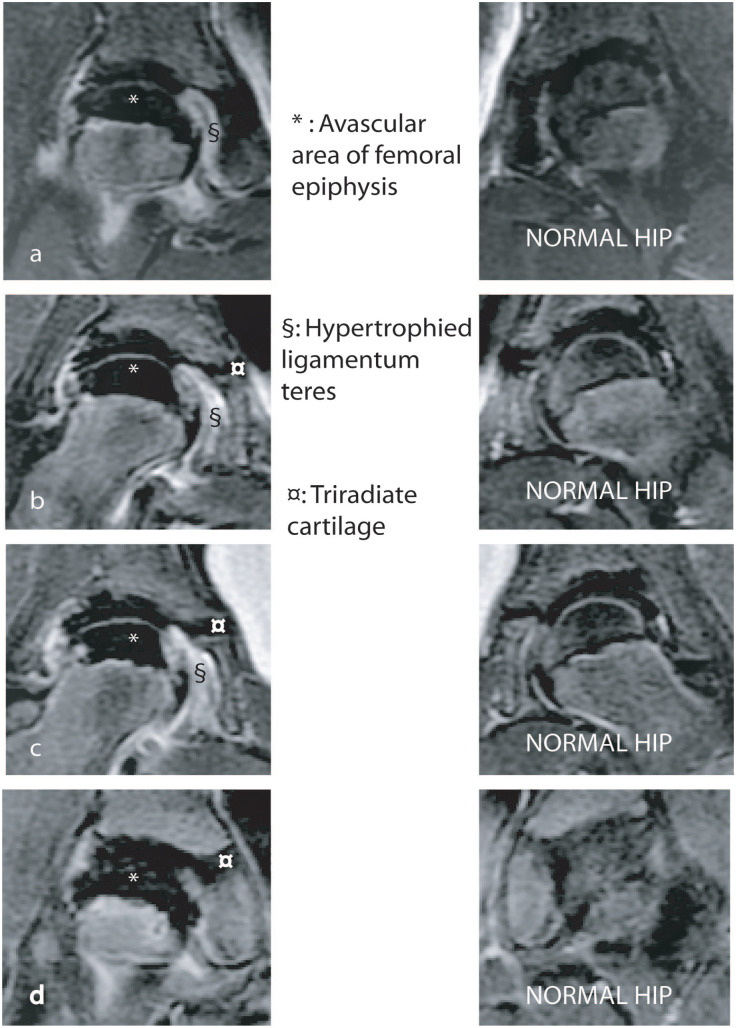
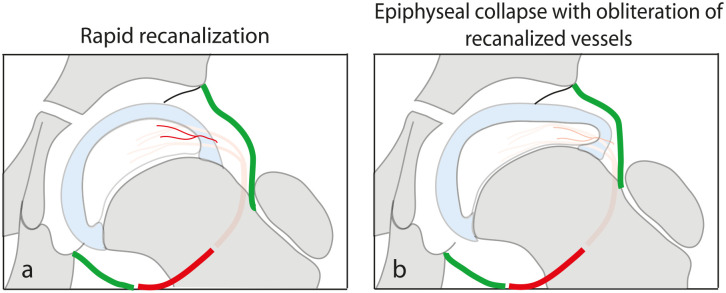
Background: Legg-Calvé-Perthes disease is a self-limiting disorder that develops in children following interruption of the blood supply to the capital femoral epiphysis. This review outlines the current knowledge on the epidemiology, natural evolution, clinical spectrum, and management of the disease.
Methods: The literature pertaining to these aspects of the disease were studied and summarized in this review.
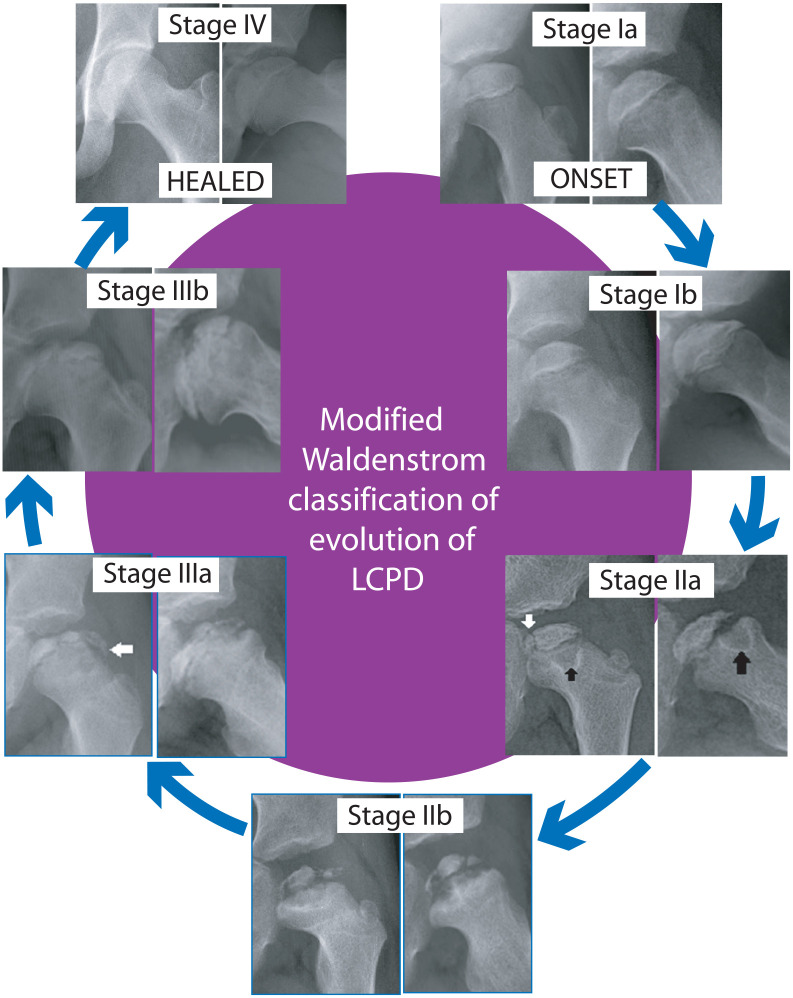
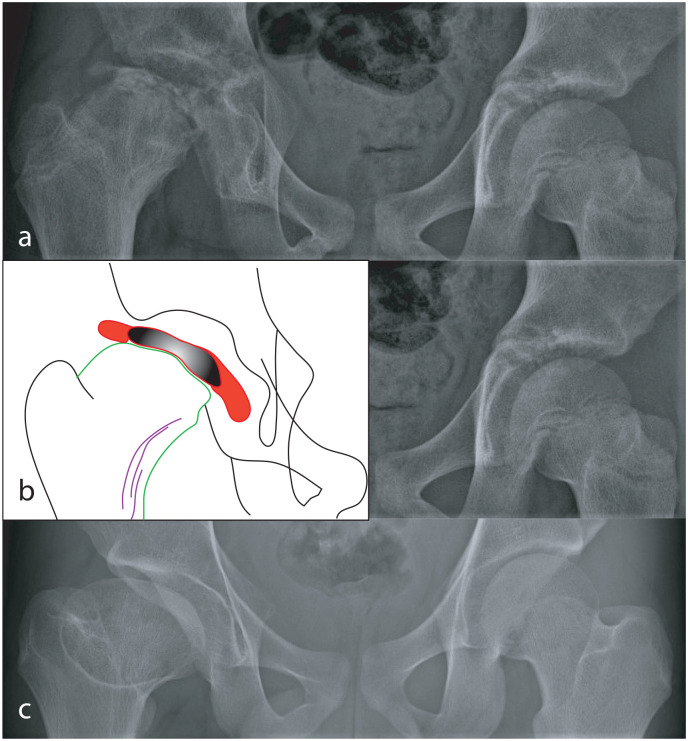
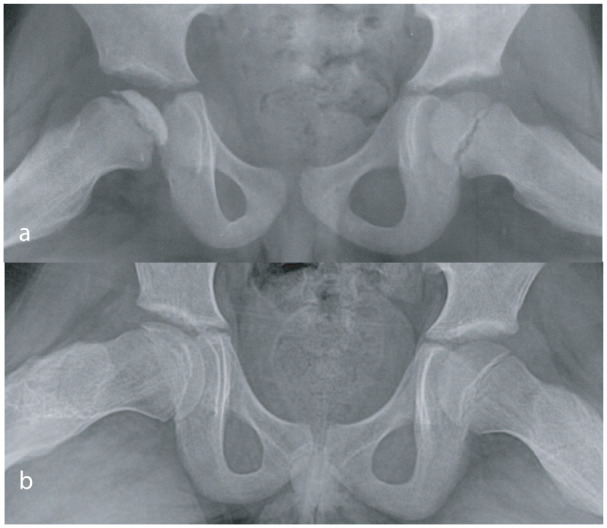
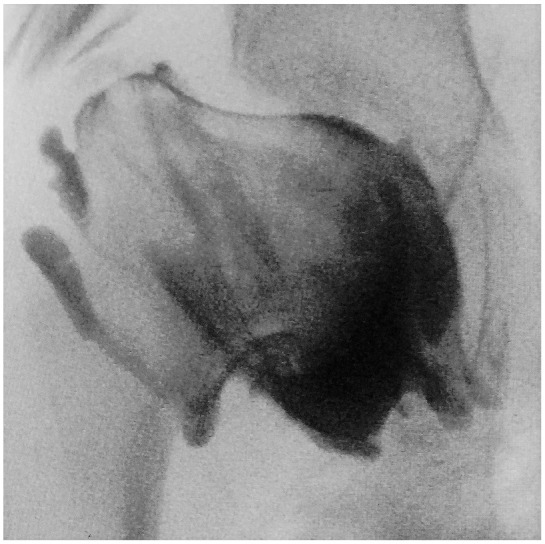
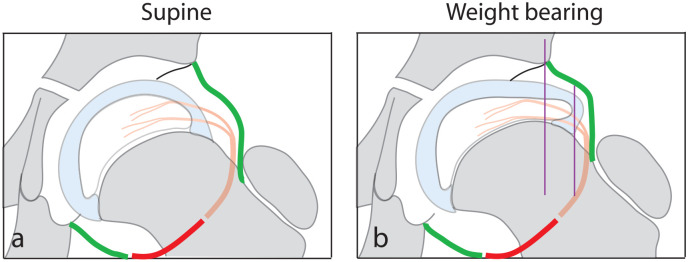
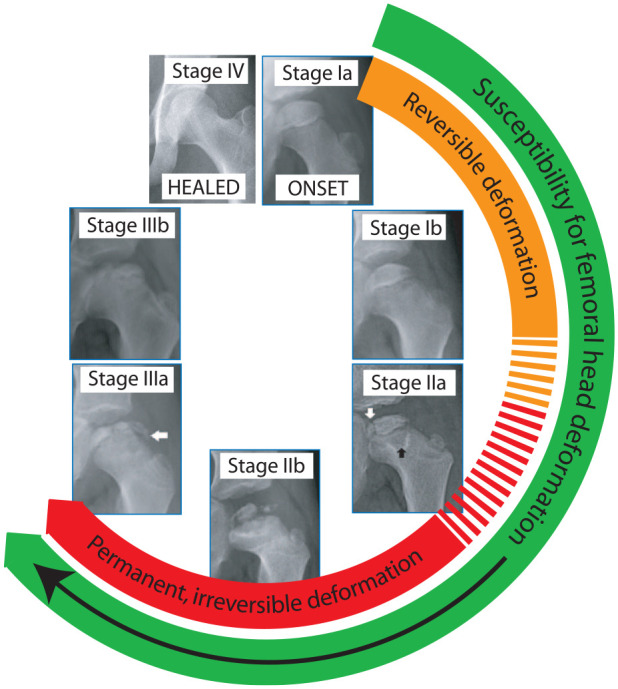
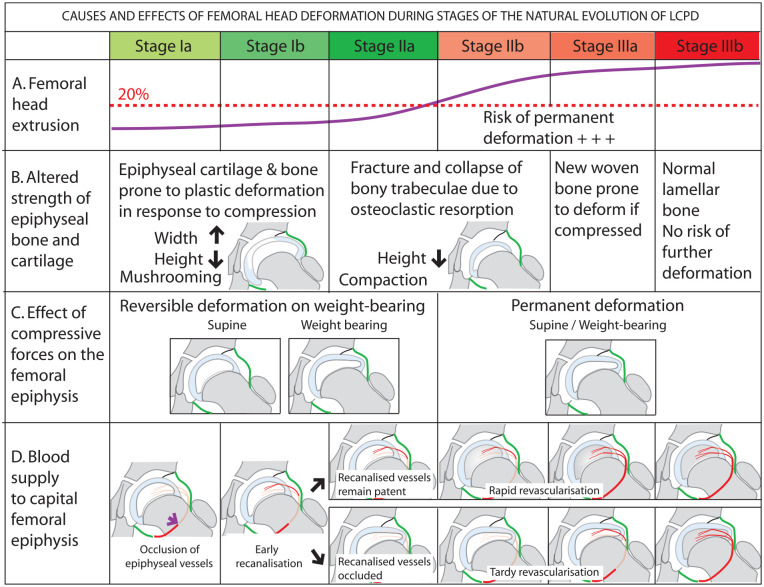
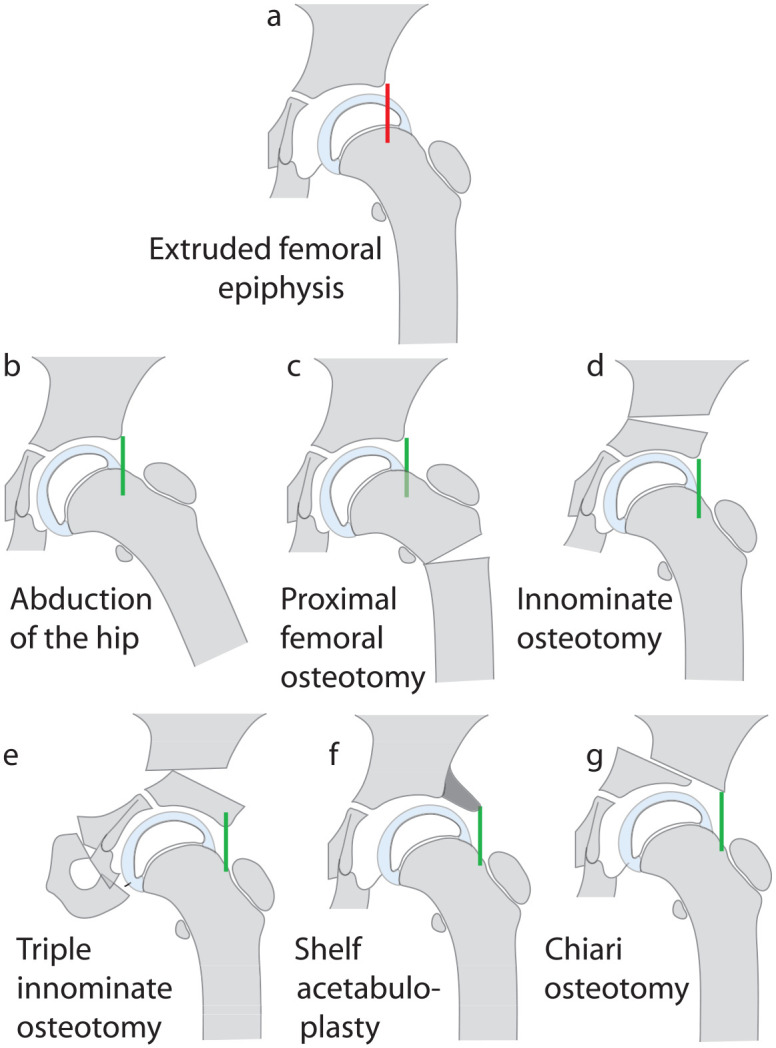
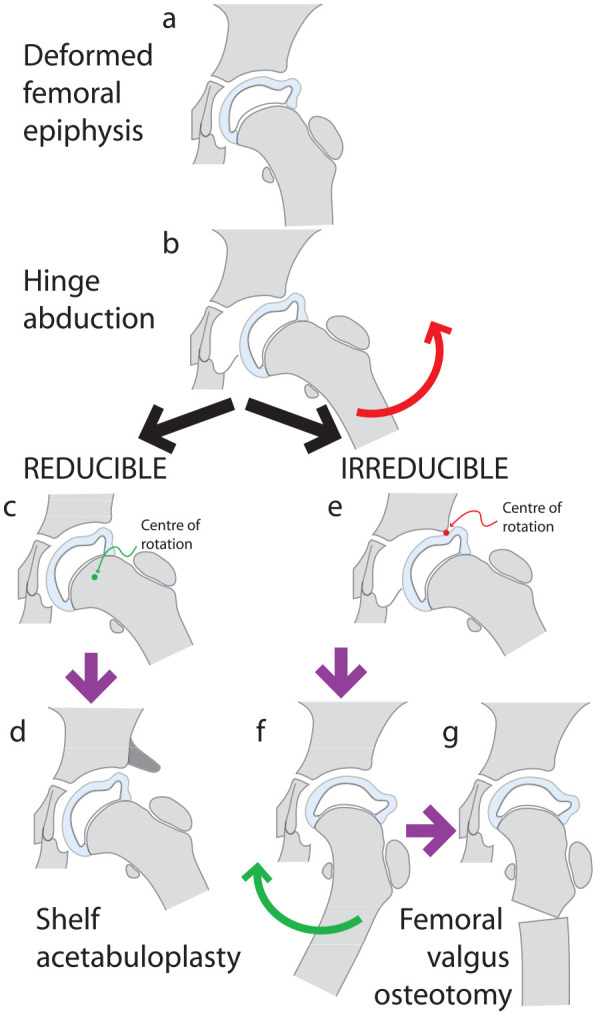
Results: Epidemiological studies suggest that environmental factors contribute to the causation of the disease. Incidence rates monitored over time indicate that the incidence of Legg-Calvé-Perthes disease is declining. The natural evolution followed on sequential plain radiographs enables division of the disease into Stages Ia, Ib, IIa, IIb, IIIa, IIIb, and IV. Reversible deformation of the capital occurs in Stages Ia-IIa simply on standing while irreversible deformation may occur in Stages IIb and IIIa. Treatment of Legg-Calvé-Perthes disease in Stages Ia-IIa aims to prevent the femoral head from getting deformed by containment and avoidance of weight-bearing. In Stages IIb and IIIa, treatment aims to remedy the effects of early irreversible deformation of the femoral head. In Stage IIIb and IV, treatment is directed to correcting the altered shape of the femoral head. The impression that these treatment methods are helpful is based on poor quality evidence.
Conclusion: There is an urgent need to undertake Level I studies to establish the efficacy of currently treatment.
Level of evidence: level V.
Keywords: Legg–Calvé–Perthes disease; containment; declining incidence; social deprivation; weight-relief.
© The Author(s) 2023.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Atsumi T, Yamano K, Muraki M, et al. The blood supply of the lateral epiphyseal arteries in Perthes’ disease. J Bone Joint Surg Br 2000; 82(3): 392–398. - PubMed
-
- Iwasaki K. The role of blood vessels within the ligamentum teres in Perthes’ disease. Clin Orthop Relat Res 1981(159): 248–256. - PubMed
-
- Inoue A, Freeman MA, Vernon-Roberts B, et al. The pathogenesis of Perthes’ disease. J Bone Joint Surg Br 1976; 58-B(4): 453–461. - PubMed
-
- Inoue A, Ono K, Takaoka K, et al. A comparative study of histology in Perthes’ disease and idiopathic avascular necrosis of the femoral head in adults (IANF). Int Orthop 1980; 4(1): 39–46. - PubMed
-
- Iwasaki K, Suzuki R, Okazaki T, et al. The haemodynamics of Perthes’ disease. An intraosseous venographic study combined with measurement of the intramedullary pressure. Int Orthop 1982; 6(3): 141–148. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
