

Diagnostic challenges and prognostic implications of extranodal extension in head and neck cancer: a state of the art review and gap analysis
- PMID: 37799466
- PMCID: PMC10548228
- DOI: 10.3389/fonc.2023.1263347
Diagnostic challenges and prognostic implications of extranodal extension in head and neck cancer: a state of the art review and gap analysis
Abstract
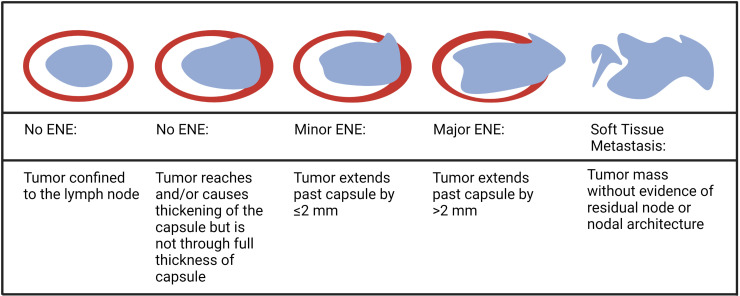
Extranodal extension (ENE) is a pattern of cancer growth from within the lymph node (LN) outward into perinodal tissues, critically defined by disruption and penetration of the tumor through the entire thickness of the LN capsule. The presence of ENE is often associated with an aggressive cancer phenotype in various malignancies including head and neck squamous cell carcinoma (HNSCC). In HNSCC, ENE is associated with increased risk of distant metastasis and lower rates of locoregional control. ENE detected on histopathology (pathologic ENE; pENE) is now incorporated as a risk-stratification factor in human papillomavirus (HPV)-negative HNSCC in the eighth edition of the American Joint Committee on Cancer (AJCC) and the Union for International Cancer Control (UICC) TNM classification. Although ENE was first described almost a century ago, several issues remain unresolved, including lack of consensus on definitions, terminology, and widely accepted assessment criteria and grading systems for both pENE and ENE detected on radiological imaging (imaging-detected ENE; iENE). Moreover, there is conflicting data on the prognostic significance of iENE and pENE, particularly in the context of HPV-associated HNSCC. Herein, we review the existing literature on ENE in HNSCC, highlighting areas of controversy and identifying critical gaps requiring concerted research efforts.
Keywords: extranodal extension; head and neck cancer; head and neck pathology; head and neck squamous cell carcinoma; locally advanced head and neck cancer.
Copyright © 2023 Henson, Abou-Foul, Morton, McDowell, Baliga, Bates, Lee, Bonomo, Szturz, Nankivell, Huang, Lydiatt, O’Sullivan and Mehanna.
Conflict of interest statement
HM reports grants from UK National Institute of Health research, Cancer Research UK, the UK Medical Research Council, and AstraZeneca; advisory board fees from AstraZeneca, MSD, Merck, Nanobiotix, and Seagen; and is Director of Warwickshire head neck clinic and Docpsert Health. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
-
- Willis RA. Epidermoid carcinoma of the head and neck, with special reference to metastasis. J Pathol Bacteriol (1930) 33(3):501–26. doi: 10.1002/path.1700330302 - DOI
-
- Routman DM, Funk RK, Tangsriwong K, Lin A, Keeney MG, Garcia JJ, et al. . Relapse rates with surgery alone in human papillomavirus-related intermediate- and high-risk group oropharynx squamous cell cancer: A multi-institutional review. Int J Radiat Oncol Biol Phys (2017) 99(4):938–46. doi: 10.1016/j.ijrobp.2017.06.2453 - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous