

Short-, Mid-, and Long-Term Efficacy of Deucravacitinib Versus Biologics and Nonbiologics for Plaque Psoriasis: A Network Meta-Analysis
- PMID: 37801281
- PMCID: PMC10613195
- DOI: 10.1007/s13555-023-01034-7
Short-, Mid-, and Long-Term Efficacy of Deucravacitinib Versus Biologics and Nonbiologics for Plaque Psoriasis: A Network Meta-Analysis
Abstract
Introduction: Deucravacitinib, a newly approved oral medication for the treatment of patients with moderate to severe plaque psoriasis, demonstrated efficacy versus apremilast and placebo in two phase 3 randomized controlled trials (RCTs). A systematic review and network meta-analysis (NMA) indirectly compared deucravacitinib with other relevant systemic biologic/nonbiologic treatments.
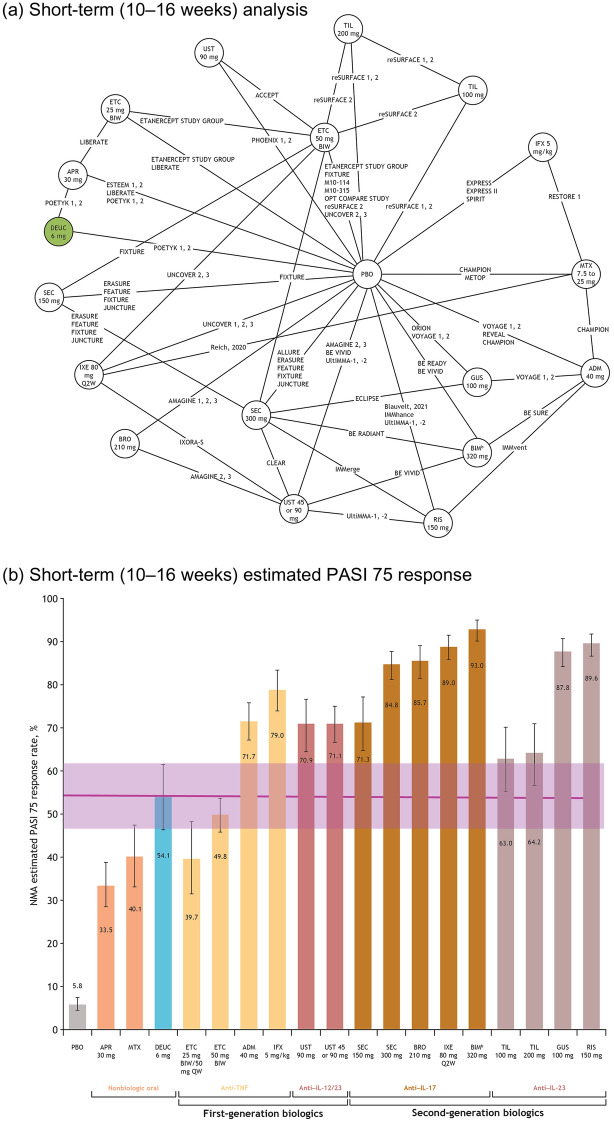
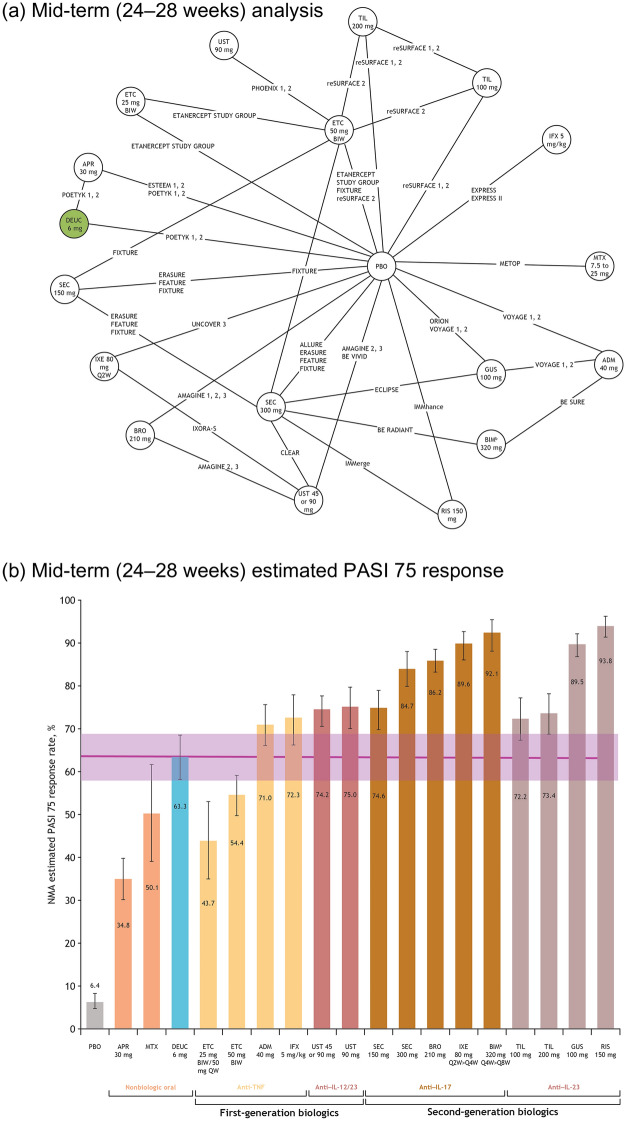
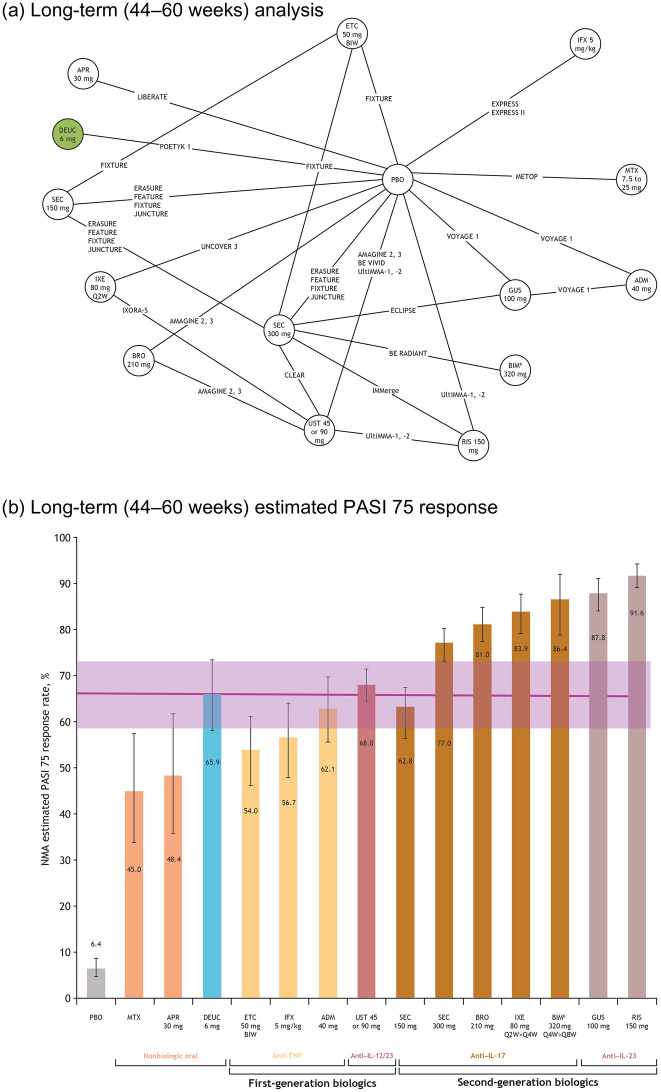
Methods: Online databases were searched for RCTs published through October 2021. Eligible studies were head-to-head comparisons between systemic therapies and/or placebo reporting 50%, 75%, 90%, or 100% improvement in Psoriasis Area and Severity Index (PASI) from baseline in adults with moderate to severe plaque psoriasis. Comparisons included tumor necrosis factor inhibitors, interleukin (IL)-17, IL-23, and IL 12/23 inhibitors, and systemic nonbiologics. A multinomial Bayesian NMA was used to derive estimates of the relative efficacy of deucravacitinib and other systemic therapies. Response probabilities for each treatment and corresponding 95% credible intervals (CrIs) for achieving a PASI response were calculated over short-, mid-, and long-term follow-up (weeks 10-16, 24-28, and 44-60).
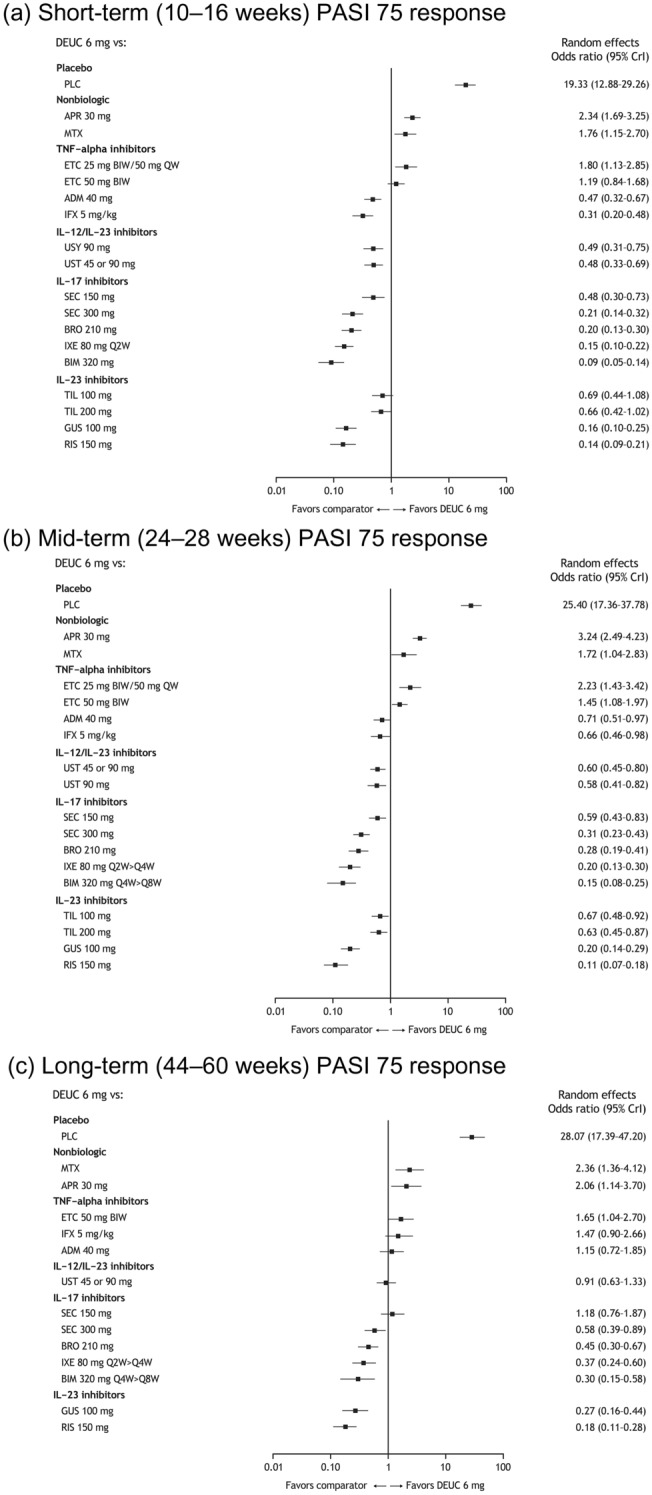
Results: The NMA included 47 RCTs. Deucravacitinib showed the highest PASI 75 response rates among nonbiologic systemic therapies across time points. Deucravacitinib PASI 75 response rate (95% CrI) over short-term follow-up was 54.1% (46.5-61.6), within the range of first-generation biologics (etanercept, 39.7% [31.6-48.3]; infliximab, 79.0% [74.0-83.5]). At mid-term follow-up, deucravacitinib PASI 75 increased to 63.3% (58.0-68.4). At long-term follow-up, deucravacitinib PASI 75 was 65.9% (58.0-73.4), comparable to first-generation biologics adalimumab (62.8%; 55.3-69.6) and ustekinumab (68.0%; 64.6-71.5).
Conclusions: Patients receiving deucravacitinib were more likely to achieve PASI 75 response versus apremilast and methotrexate across all time points. The long-term PASI 75 response rate for deucravacitinib was similar to those of adalimumab and ustekinumab. The approval of deucravacitinib offers patients the choice of an oral therapy with long-term efficacy similar to that of some biologics.
Keywords: Biologics; Deucravacitinib; Indirect treatment comparison; Network meta-analysis; Non-biologics; Psoriasis.
© 2023. The Author(s).
Conflict of interest statement
April W. Armstrong has received grants and personal fees from AbbVie, Bristol Myers Squibb, Eli Lilly, Janssen, Leo Pharma, and Novartis; personal fees from Boehringer Ingelheim/Parexel, Celgene, Dermavant, Genentech, GlaxoSmithKline, Menlo Therapeutics, Merck, Modernizing Medicine, Ortho Dermatologics, Pfizer, Regeneron, Sanofi Genzyme, Science 37, Sun Pharma, and Valeant, and grants from Dermira, Kyowa Hakko Kirin, and UCB. Richard Warren has received research grants from AbbVie, Almirall, Amgen, Celgene, Eli Lilly, Janssen, Leo Pharma, Novartis, Pfizer, and UCB; and consulting fees from AbbVie, Almirall, Amgen, Biogen, Boehringer Ingelheim, Celgene, DiCE, Eli Lilly, Janssen, Leo Pharma, Novartis, Pfizer, Sanofi, UCB, and Union. Yichen Zhong, Joe Zhuo, Renata Kisa, and Carolin Daamen are employees of and shareholders in Bristol Myers Squibb. Allie Cichewicz, Ananth Kadambi, Daniela Junqueira, and Tracy Westley are employed by Evidera, a part of Thermo Fisher Scientific, a company that provides consulting and other research services to Bristol Myers Squibb. Matthias Augustin has served on advisory boards for AbbVie, Amgen, Boehringer Ingelheim, Janssen Biotech, and Leo Pharma; has received consulting fees from AbbVie, Amgen, Eli Lilly, Janssen Biotech, Leo Pharma, Novartis, Sun Pharma, and UCB; has received honoraria from AbbVie, Amgen, Boehringer Ingelheim, Eli Lilly, Janssen Biotech, Leo Pharma, Novartis, Sun Pharma, and UCB; has served as an investigator for AbbVie, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Janssen Biotech, Leo Pharma, Merck, Novartis, Sun Pharma, and UCB; has received research grants from AbbVie, Amgen, Boehringer Ingelheim, Celgene, Janssen Biotech, Leo Pharma, Merck, and Sun Pharma; and has served as a speaker for AbbVie, Amgen, Janssen Biotech, Leo Pharma, Sun Pharma, and UCB.
Figures
References
-
- Armstrong AW, Gooderham M, Warren RB, et al. Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: efficacy and safety results from the 52-week, randomized, double-blinded, placebo-controlled phase 3 POETYK PSO-1 trial. J Am Acad Dermatol. 2023;88(1):29–39. doi: 10.1016/j.jaad.2022.07.002. - DOI - PubMed
-
- Strober B, Thaçi D, Sofen H, et al. Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: efficacy and safety results from the 52-week, randomized, double-blinded, Program fOr Evaluation of TYK2 inhibitor psoriasis second phase 3 trial. J Am Acad Dermatol. 2023;88(1):40–51. doi: 10.1016/j.jaad.2022.08.061. - DOI - PubMed
-
- Gordon KB, Strober B, Lebwohl M, et al. Efficacy and safety of risankizumab in moderate-to-severe plaque psoriasis (UltIMMa-1 and UltIMMa-2): results from two double-blind, randomised, placebo-controlled and ustekinumab-controlled phase 3 trials. Lancet. 2018;392(10148):650–661. doi: 10.1016/S0140-6736(18)31713-6. - DOI - PubMed
LinkOut - more resources
Full Text Sources
