

Patritumab Deruxtecan (HER3-DXd), a Human Epidermal Growth Factor Receptor 3-Directed Antibody-Drug Conjugate, in Patients With Previously Treated Human Epidermal Growth Factor Receptor 3-Expressing Metastatic Breast Cancer: A Multicenter, Phase I/II Trial
- PMID: 37801674
- PMCID: PMC10730028
- DOI: 10.1200/JCO.23.00882
Patritumab Deruxtecan (HER3-DXd), a Human Epidermal Growth Factor Receptor 3-Directed Antibody-Drug Conjugate, in Patients With Previously Treated Human Epidermal Growth Factor Receptor 3-Expressing Metastatic Breast Cancer: A Multicenter, Phase I/II Trial
Abstract
Purpose: Human epidermal growth factor receptor 3 (HER3) is broadly expressed in breast cancer; high expression is associated with an adverse prognosis. Patritumab deruxtecan (HER3-DXd) is an investigational HER3-targeted antibody-drug conjugate that is being evaluated as a novel treatment in HER3-expressing advanced breast cancer in the U31402-A-J101 study.
Methods: Adults with disease progression on previous therapies were eligible. Patients in the dose-escalation, dose-finding, and dose-expansion parts received HER3-DXd 1.6-8.0 mg/kg intravenously once every 3 weeks or one of two alternative dosing regimens. In the dose-escalation part, the primary objectives were to determine the maximum tolerated dose and recommended dose for expansion (RDE). The safety and efficacy of the RDE were assessed during dose expansion.
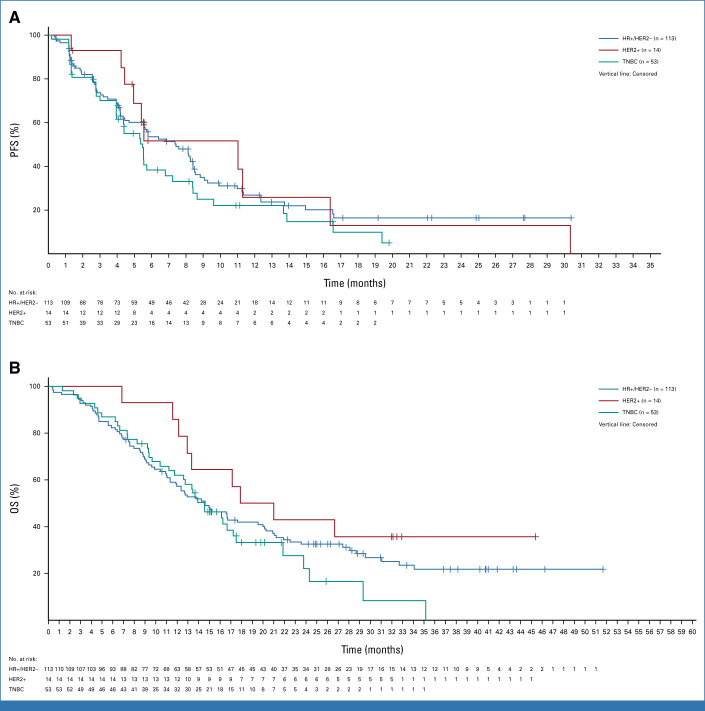
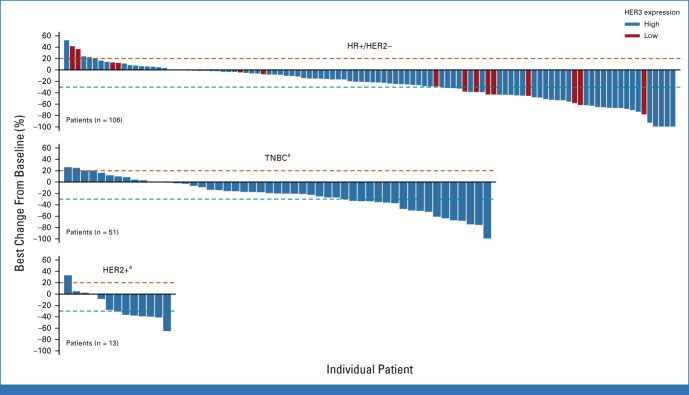
Results: One hundred eighty-two enrolled patients received ≥1 dose of HER3-DXd. Patients had a median of five previous therapies for advanced disease. Efficacy results are reported across clinical subtypes: hormone receptor-positive (HR+)/human epidermal growth factor receptor 2-negative (HER2-negative) breast cancer (n = 113; objective response rate [ORR], 30.1%; median progression-free survival [mPFS], 7.4 months), triple-negative breast cancer (n = 53; ORR, 22.6%; mPFS, 5.5 months), and HER2-positive breast cancer (n = 14; ORR, 42.9%; mPFS, 11.0 months). Objective responses were observed in cancers with HER3-high and HER3-low membrane expression. Dose-limiting toxicities observed during dose selection were decreased platelet count and elevated aminotransferases. In dose expansion, GI and hematologic toxicities were the most common treatment-emergent adverse events (TEAEs) observed. Grade ≥3 TEAEs were observed in 71.4% of patients, and 9.9% discontinued treatment because of TEAEs. Three grade 3 and one grade 5 treatment-related interstitial lung disease events occurred.
Conclusion: HER3-DXd demonstrated a manageable safety profile and durable efficacy in heavily pretreated patients across clinical subtypes. These data warrant further evaluation of HER3-DXd in patients with HER3-expressing metastatic breast cancer.
Trial registration: ClinicalTrials.gov NCT02980341.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
No other potential conflicts of interest were reported.
Figures
References
-
- Chiu CG, Masoudi H, Leung S, et al. : HER-3 overexpression is prognostic of reduced breast cancer survival: A study of 4046 patients. Ann Surg 251:1107-1116, 2010 - PubMed
-
- Ocana A, Vera-Badillo F, Seruga B, et al. : HER3 overexpression and survival in solid tumors: A meta-analysis. J Natl Cancer Inst 105:266-273, 2013 - PubMed
-
- Witton CJ, Reeves JR, Going JJ, et al. : Expression of the HER1-4 family of receptor tyrosine kinases in breast cancer. J Pathol 200:290-297, 2003 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
