

Ultrasonographic criteria in the diagnosis of polycystic ovary syndrome: a systematic review and diagnostic meta-analysis
- PMID: 37804097
- PMCID: PMC10762001
- DOI: 10.1093/humupd/dmad027
Ultrasonographic criteria in the diagnosis of polycystic ovary syndrome: a systematic review and diagnostic meta-analysis
Abstract
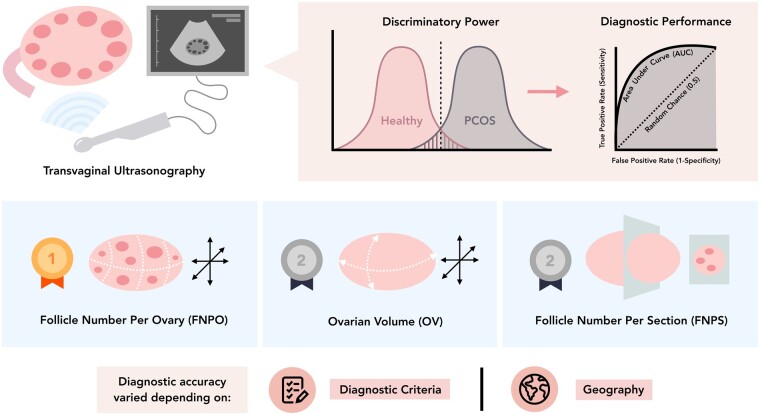
Background: Polycystic ovary morphology (PCOM) on ultrasonography is considered as a cardinal feature of polycystic ovarian syndrome (PCOS). Its relevance as a diagnostic criterion for PCOS was reaffirmed in the most recent International Evidence-Based Guideline for the Assessment and Management of PCOS. However, there remains a lack of clarity regarding the best practices and specific ultrasonographic markers to define PCOM.
Objective and rationale: The aim of this systematic review and diagnostic meta-analysis was to assess the diagnostic accuracy of various ultrasonographic features of ovarian morphology in the diagnosis of PCOS.
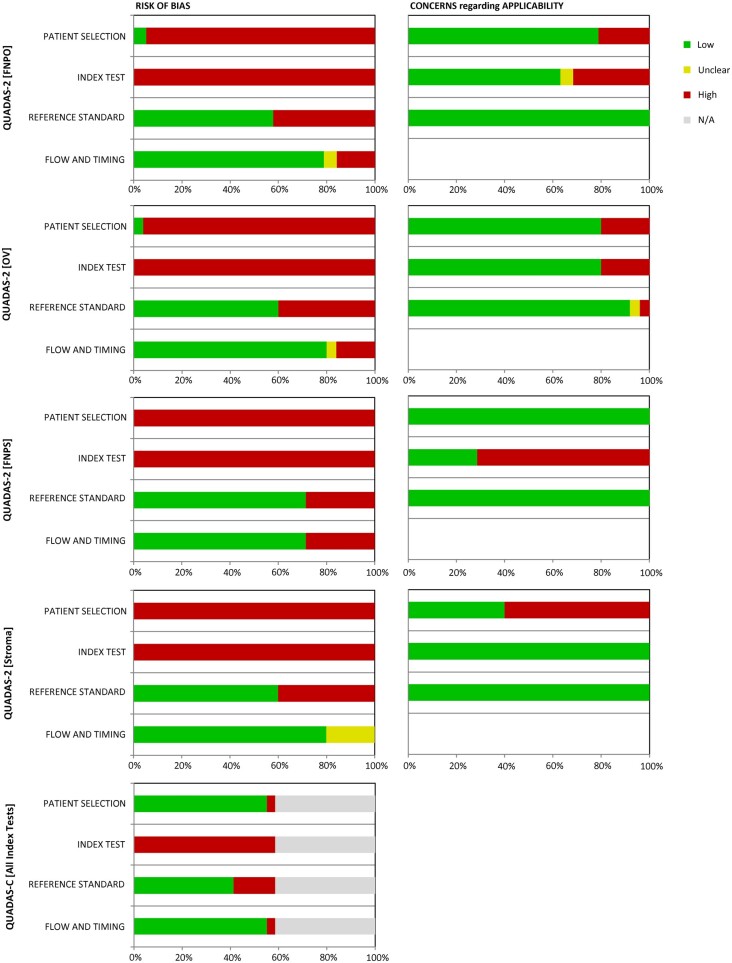
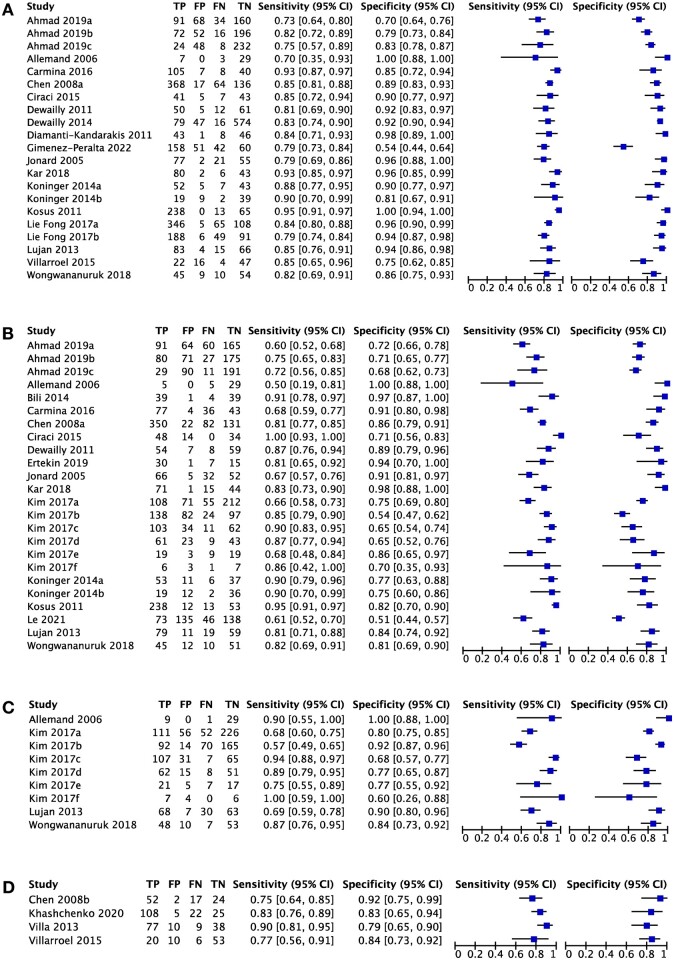
Search methods: Relevant studies published from 1 January 1990 to 12 June 2023 were identified by a systematic search in PubMed, Web of Science, Scopus, CINAHL, and CENTRAL. Studies that generated diagnostic accuracy measures (e.g. proposed thresholds, sensitivity, specificity) for PCOS using the following ultrasonographic markers met criteria for inclusion: follicle number per ovary (FNPO) or per single cross-section (FNPS), ovarian volume (OV), and stromal features. Studies on pregnant or post-menopausal women were excluded. Risk of bias and applicability assessment for diagnostic test accuracy studies were determined using the QUADAS-2 and QUADAS-C tool for a single index test or between multiple index tests, respectively. Diagnostic meta-analysis was conducted using a bivariate model of pooled sensitivity and specificity, and visualized using forest plots and summary receiver-operating characteristic (SROC) curves.
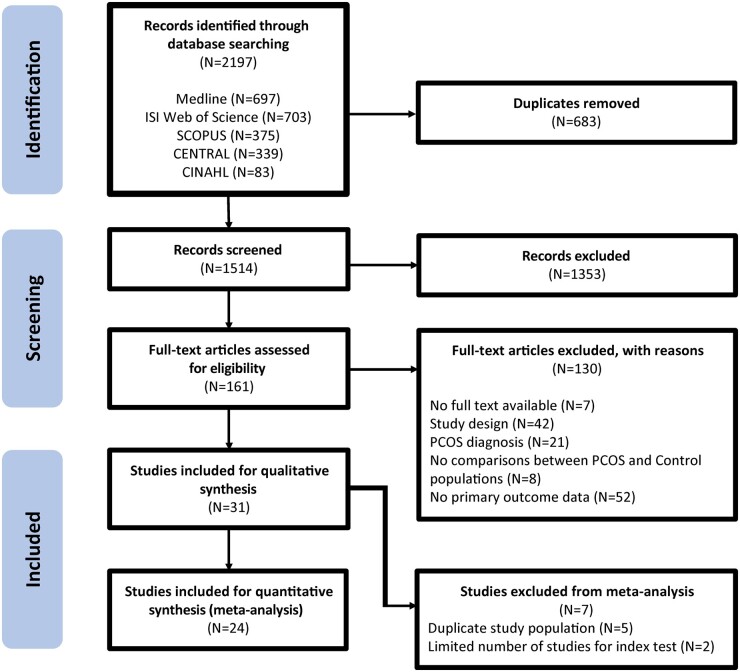
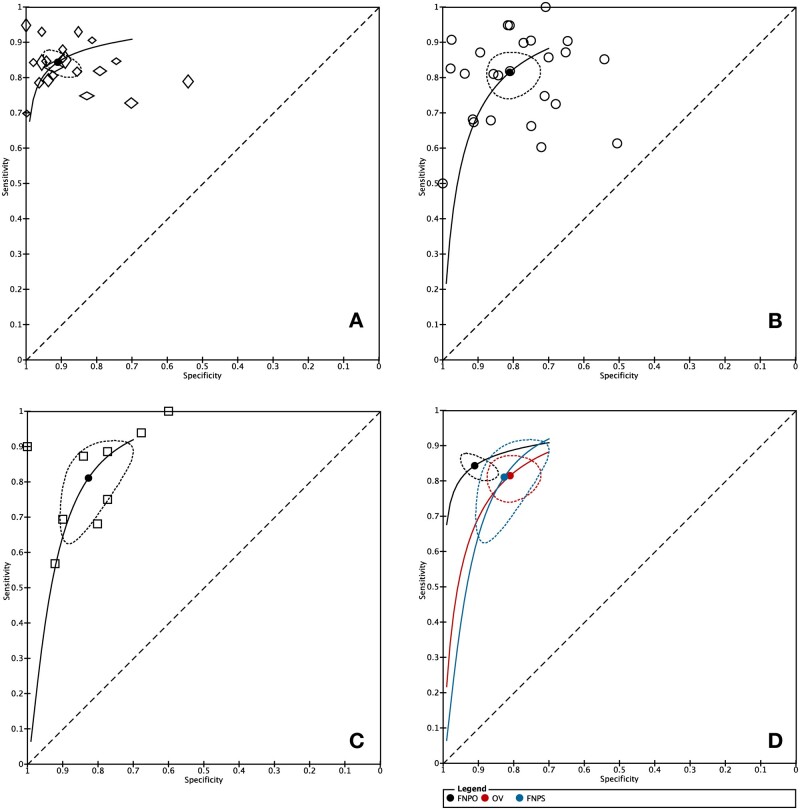
Outcomes: From a total of 2197 records initially identified, 31 studies were included. Data from five and two studies were excluded from the meta-analysis due to duplicate study populations or limited data for the index test, leaving 24 studies. Pooled results of 20 adult studies consisted of 3883 control participants and 3859 individuals with PCOS. FNPO was the most accurate diagnostic marker (sensitivity: 84%, CI: 81-87%; specificity: 91%, CI: 86-94%; AUC: 0.905) in adult women. OV and FNPS had similar pooled sensitivities (OV: 81%, CI: 76-86%; FNPS: 81%, CI: 70-89%) but inferior pooled specificities (OV: 81%, CI: 75-86%; FNPS: 83%, CI: 75-88%) and AUCs (OV: 0.856; FNPS: 0.870) compared to FNPO. Pooled results from four adolescent studies consisting of 210 control participants and 268 girls with PCOS suggested that OV may be a robust ultrasonographic marker for PCOS diagnosis albeit the current evidence remains limited. The majority of the studies had high risk of bias for the patient selection (e.g. lack of randomized/consecutive patient selection) and index test (e.g. lack of pre-proposed thresholds for comparison) domains across all ultrasonographic markers. As such, diagnostic meta-analysis was unable to determine the most accurate cutoff for ultrasonographic markers to diagnose PCOS. Subgroup analysis suggested that stratification based on previously proposed diagnostic thresholds, age, BMI, or technology did not account for the heterogeneity in diagnostic accuracy observed across the studies. Studies that diagnosed PCOS using the Rotterdam criteria had improved sensitivity for FNPO. Studies from North America had lower diagnostic accuracy when compared to Asian studies (FNPO: sensitivity) and European studies (OV: specificity, diagnostic odds ratio and positive likelihood ratio). Geographic differences in diagnostic accuracy may potentially be due to differences in age, BMI, and diagnostic criteria of the PCOS group across regions.
Wider implications: This diagnostic meta-analysis supports the use of FNPO as the gold standard in the ultrasonographic diagnosis of PCOS in adult women. OV and FNPS provide alternatives if total antral follicle counts cannot be accurately obtained. Our findings support the potential for ultrasonographic evidence of PCOM in adolescents as more data becomes available. Subgroup analysis suggests the need to investigate any relative contributions of geographical differences on PCOS phenotypes. These findings may provide the basis for the development of strategies and best practices toward a standardized definition of PCOM and a more accurate ultrasonographic evaluation of PCOS.
Keywords: diagnostic imaging; ovarian follicle; ovary; polycystic ovary syndrome; ultrasonography.
© The Author(s) 2023. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
The authors have no conflict of interest to disclose.
Figures
References
-
- Ahmad AK, Kao CN, Quinn M, Lenhart N, Rosen M, Cedars MI, Huddleston H.. Differential rate in decline in ovarian reserve markers in women with polycystic ovary syndrome compared with control subjects: results of a longitudinal study. Fertil Steril 2018;109:526–531. - PubMed
-
- Ahmad AK, Quinn M, Kao CN, Greenwood E, Cedars MI, Huddleston HG.. Improved diagnostic performance for the diagnosis of polycystic ovary syndrome using age-stratified criteria. Fertil Steril 2019;111:787–793.e2. - PubMed
-
- Allemand MC, Tummon IS, Phy JL, Foong SC, Dumesic DA, Session DR.. Diagnosis of polycystic ovaries by three-dimensional transvaginal ultrasound. Fertil Steril 2006;85:214–219. - PubMed
-
- Azziz R, Carmina E, Chen Z, Dunaif A, Laven JSE, Legro RS, Lizneva D, Natterson-Horowtiz B, Teede HJ, Yildiz BO.. Polycystic ovary syndrome. Nat Rev Dis Primers 2016;2:16057–16018. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
