

Mavacamten: a first-in-class myosin inhibitor for obstructive hypertrophic cardiomyopathy
- PMID: 37804245
- PMCID: PMC10659958
- DOI: 10.1093/eurheartj/ehad637
Mavacamten: a first-in-class myosin inhibitor for obstructive hypertrophic cardiomyopathy
Erratum in
-
Correction to: Mavacamten: a first-in-class myosin inhibitor for obstructive hypertrophic cardiomyopathy.Eur Heart J. 2024 Jan 27;45(4):286. doi: 10.1093/eurheartj/ehad854. Eur Heart J. 2024. PMID: 38108764 Free PMC article. No abstract available.
Abstract
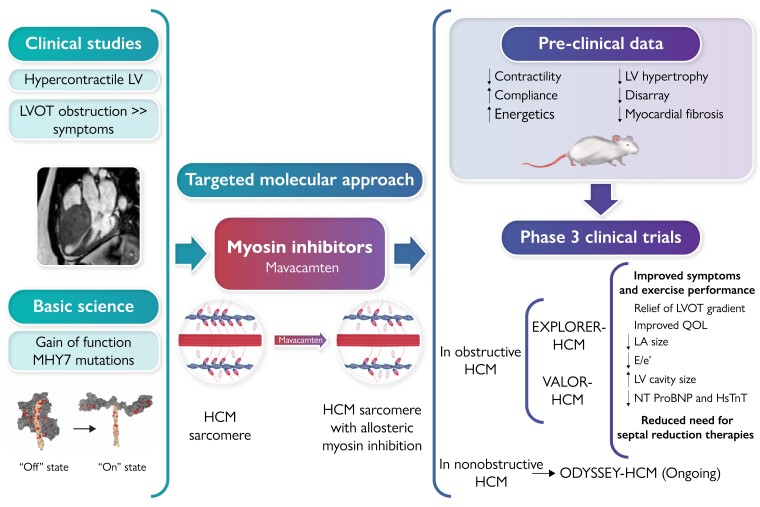
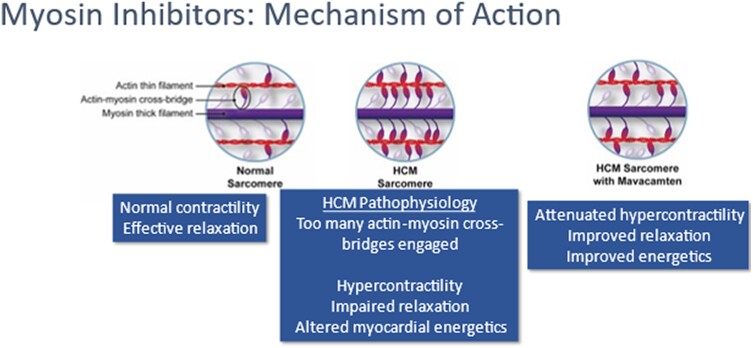
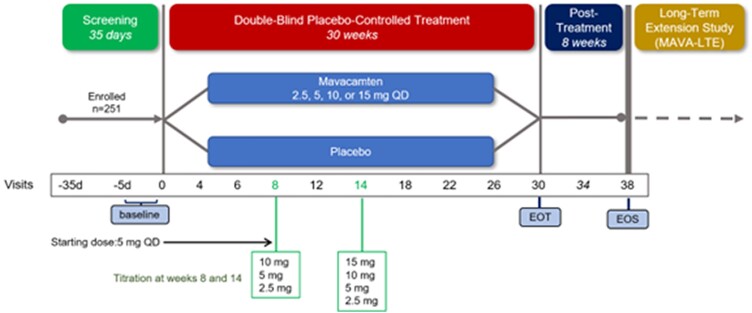
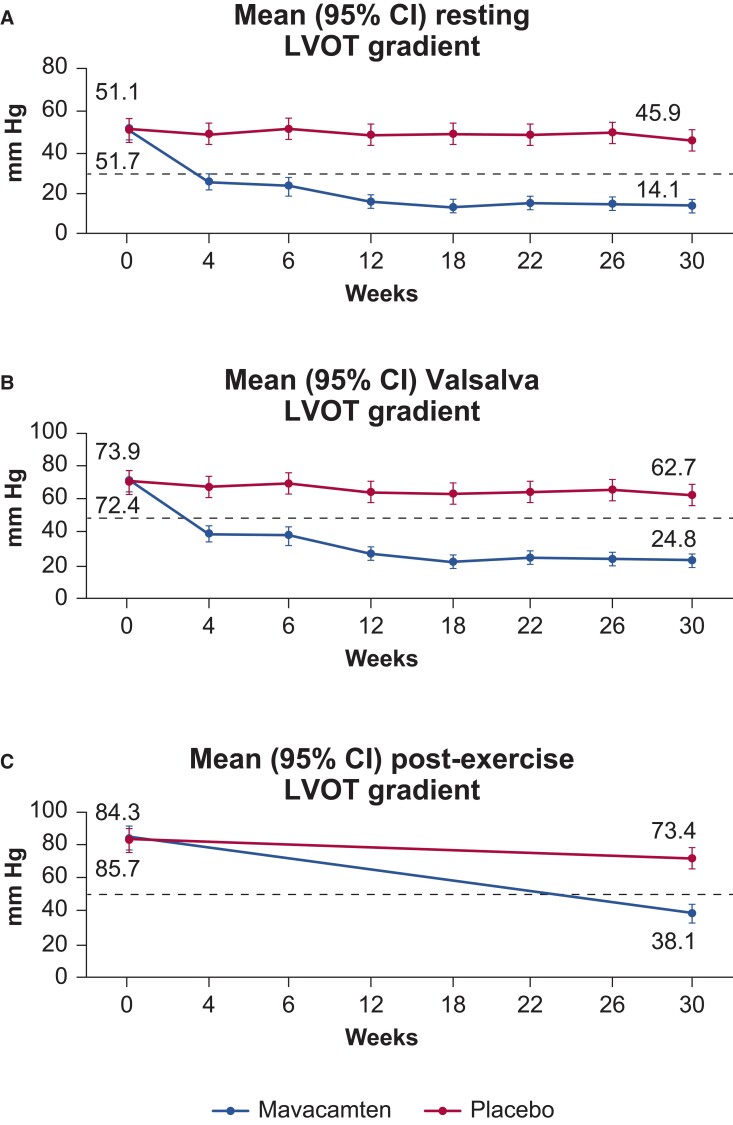
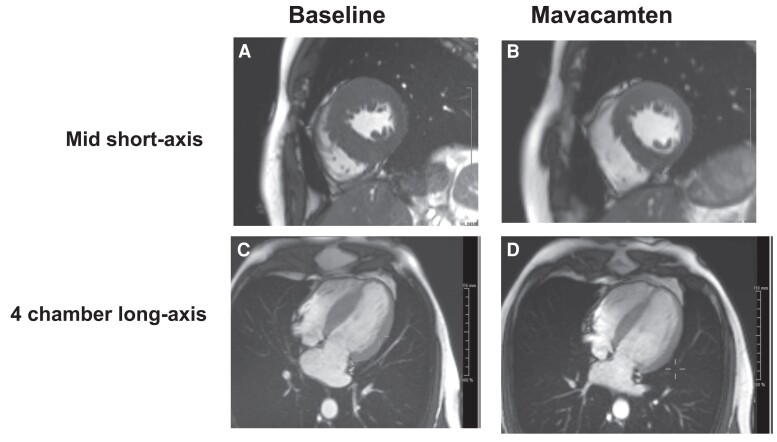
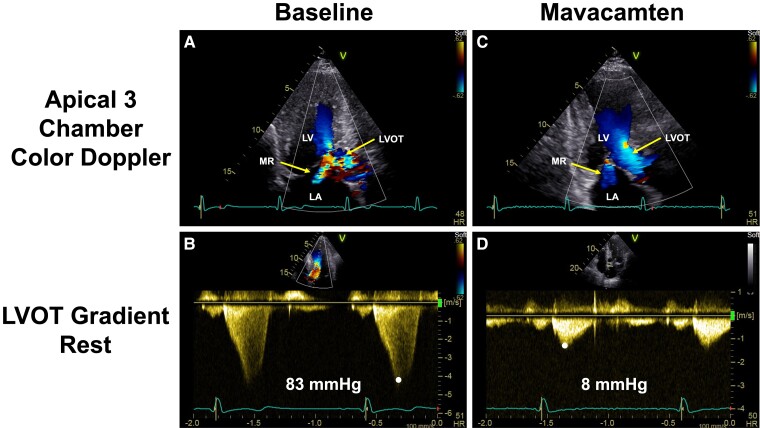
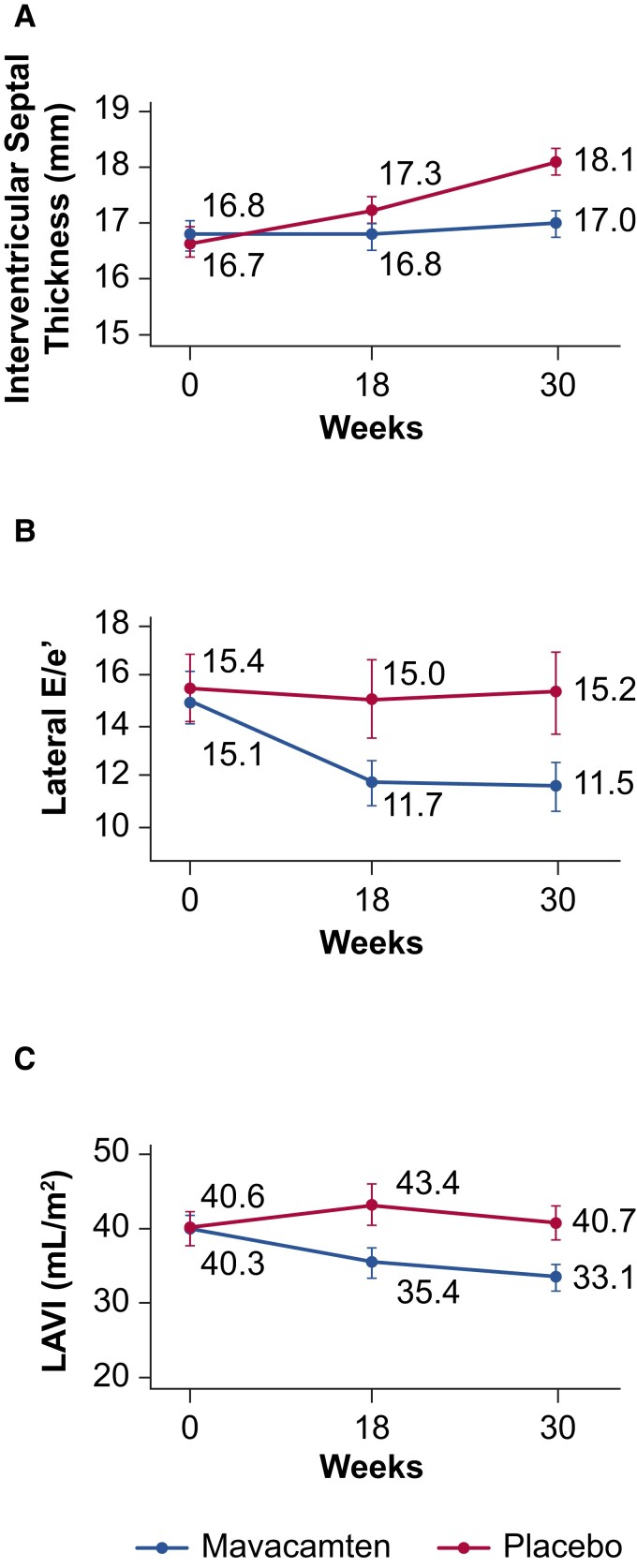
Mavacamten is a first-in-class, targeted, cardiac-specific myosin inhibitor approved by the US Food and Drug Administration for the treatment of adults with symptomatic New York Heart Association Classes II and III obstructive hypertrophic cardiomyopathy (oHCM). Mavacamten was developed to target the hyper-contractile phenotype, which plays a critical role in the pathophysiology of the disease. In Phase 2 and 3 clinical trials, mavacamten was well tolerated, reduced left ventricular outflow tract gradients, improved exercise capacity and symptoms, and was associated with improvements in other clinically relevant parameters, such as patient-reported outcomes and circulating biomarkers. In addition, treatment with mavacamten was associated with evidence of favourable cardiac remodelling in multi-modality imaging studies. Mavacamten substantially reduced guideline eligibility for septal reduction therapy candidates with oHCM and drug-refractory symptoms. In this article, the available efficacy and safety data from completed and ongoing clinical studies of mavacamten in patients with symptomatic oHCM are reviewed. Longer term extension studies may help address questions related to the positioning of mavacamten in current oHCM management algorithms, interactions with background therapy, as well as the potential for disease modification beyond symptomatic relief of left ventricular outflow tract obstruction.
Keywords: Ejection fraction; Myectomy; Myosin; Pressure gradient.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Ommen SR, Mital S, Burke MA, Day SM, Deswal A, Elliott P et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation 2020;142:e558–631. 10.1161/CIR.0000000000000937 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
