Identification of post-cardiac arrest blood pressure thresholds associated with outcomes in children: an ICU-Resuscitation study
- PMID: 37805481
- PMCID: PMC10559632
- DOI: 10.1186/s13054-023-04662-9
Identification of post-cardiac arrest blood pressure thresholds associated with outcomes in children: an ICU-Resuscitation study
Abstract
Introduction: Though early hypotension after pediatric in-hospital cardiac arrest (IHCA) is associated with inferior outcomes, ideal post-arrest blood pressure (BP) targets have not been established. We aimed to leverage prospectively collected BP data to explore the association of post-arrest BP thresholds with outcomes. We hypothesized that post-arrest systolic and diastolic BP thresholds would be higher than the currently recommended post-cardiopulmonary resuscitation BP targets and would be associated with higher rates of survival to hospital discharge.
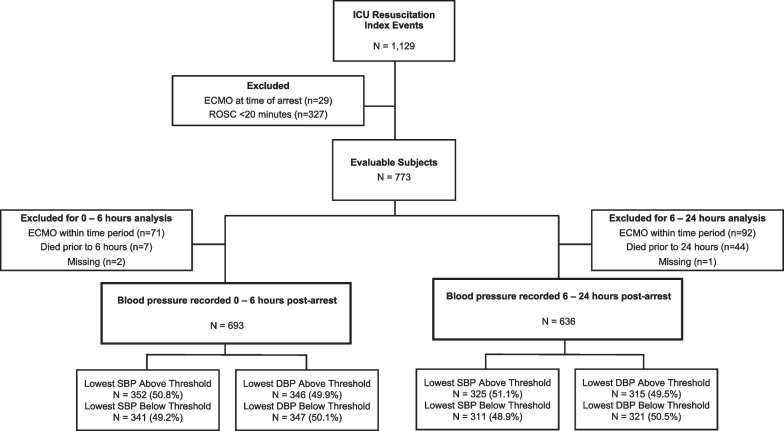
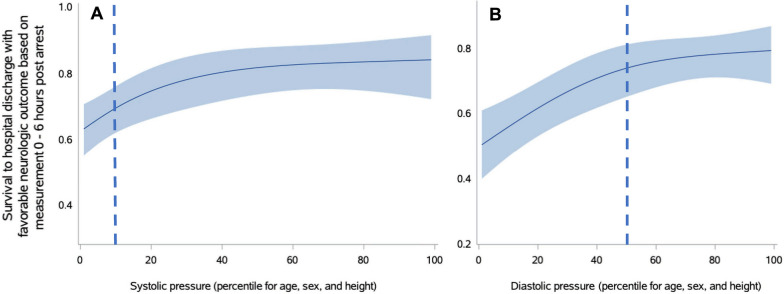
Methods: We performed a secondary analysis of prospectively collected BP data from the first 24 h following return of circulation from index IHCA events enrolled in the ICU-RESUScitation trial (NCT02837497). The lowest documented systolic BP (SBP) and diastolic BP (DBP) were percentile-adjusted for age, height and sex. Receiver operator characteristic curves and cubic spline analyses controlling for illness category and presence of pre-arrest hypotension were generated exploring the association of lowest post-arrest SBP and DBP with survival to hospital discharge and survival to hospital discharge with favorable neurologic outcome (Pediatric Cerebral Performance Category of 1-3 or no change from baseline). Optimal cutoffs for post-arrest BP thresholds were based on analysis of receiver operator characteristic curves and spline curves. Logistic regression models accounting for illness category and pre-arrest hypotension examined the associations of these thresholds with outcomes.
Results: Among 693 index events with 0-6 h post-arrest BP data, identified thresholds were: SBP > 10th percentile and DBP > 50th percentile for age, sex and height. Fifty-one percent (n = 352) of subjects had lowest SBP above threshold and 50% (n = 346) had lowest DBP above threshold. SBP and DBP above thresholds were each associated with survival to hospital discharge (SBP: aRR 1.21 [95% CI 1.10, 1.33]; DBP: aRR 1.23 [1.12, 1.34]) and survival to hospital discharge with favorable neurologic outcome (SBP: aRR 1.22 [1.10, 1.35]; DBP: aRR 1.27 [1.15, 1.40]) (all p < 0.001).
Conclusions: Following pediatric IHCA, subjects had higher rates of survival to hospital discharge and survival to hospital discharge with favorable neurologic outcome when BP targets above a threshold of SBP > 10th percentile for age and DBP > 50th percentile for age during the first 6 h post-arrest.
Keywords: Blood pressure; Cardiopulmonary resuscitation; Hypotension; Infant; Neonatal; Outcomes; Pediatric; Post-cardiac arrest.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
Drs. Reeder’s, Carcillo’s, Carpenter’s, Dean’s, Fink’s, Frazier’s, Friess’, Hall’s, Manga’s, Morgan’s, Mourani’s, Nadkarni’s, Naim’s, Palmer’s, Pollack’s, Wessel’s, Wolfe’s, Yates’, Zuppa’s, Sutton’s, and Meert’s institutions received funding from the National Institutes of Health (NIH). Drs. Reeder, Berg, Carcillo, Carpenter, Dean, Fink, Frazier, Friess, Hall, Horvat, Maa, McQuillen, Meert, Morgan, Mourani, Nadkarni, Naim, Pollack, Wessel, Wolfe, Yates, and Zuppa received support for article research from the NIH. Dr. Berg’s institution received funding from the National Institute of Child Health and Human Development (NICHD) Collaborative Pediatric Critical Care Research Network grant and the National Heart, Lung, and Blood Institute (NHLBI)
Figures