

Cerebral oximetry monitoring versus usual care for extremely preterm infants: a study protocol for the 2-year follow-up of the SafeBoosC-III randomised clinical trial
- PMID: 37805539
- PMCID: PMC10560418
- DOI: 10.1186/s13063-023-07653-x
Cerebral oximetry monitoring versus usual care for extremely preterm infants: a study protocol for the 2-year follow-up of the SafeBoosC-III randomised clinical trial
Abstract
Background: In the SafeBoosC-III trial, treatment guided by cerebral oximetry monitoring for the first 72 hours after birth did not reduce the incidence of death or severe brain injury in extremely preterm infants at 36 weeks' postmenstrual age, as compared with usual care. Despite an association between severe brain injury diagnosed in the neonatal period and later neurodevelopmental disability, this relationship is not always strong. The objective of the SafeBoosC-III follow-up study is to assess mortality, neurodevelopmental disability, or any harm in trial participants at 2 years of corrected age. One important challenge is the lack of funding for local costs for a trial-specific assessment.
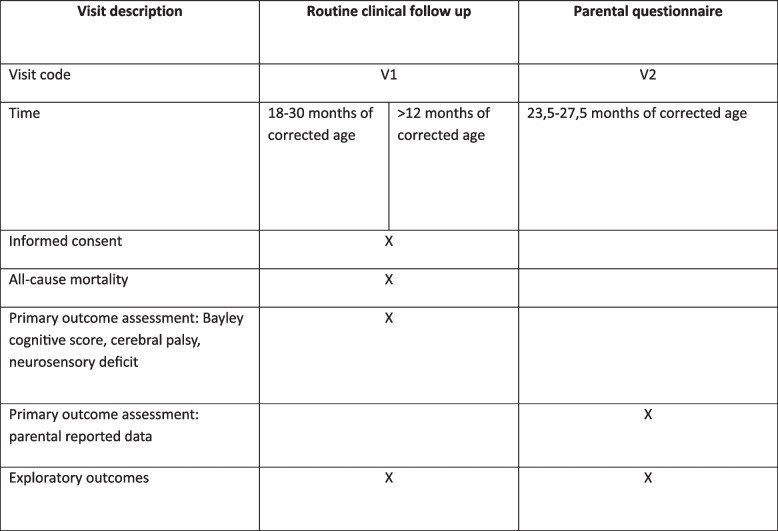
Methods: Of the 1601 infants randomised in the SafeBoosC-III trial, 1276 infants were alive at 36 weeks' postmenstrual age and will potentially be available for the 2-year follow-up. Inclusion criteria will be enrollment in a neonatal intensive care unit taking part in the follow-up study and parental consent if required by local regulations. We aim to collect data from routine follow-up programmes between the ages of 18 and 30 months of corrected age. If no routine follow-up has been conducted, we will collect informal assessments from other health care records from the age of at least 12 months. A local co-investigator blinded to group allocation will classify outcomes based on these records. We will supplement this with parental questionnaires including the Parent Report of Children's Abilities-Revised. There will be two co-primary outcomes: the composite of death or moderate or severe neurodevelopmental disability and mean Bayley-III/IV cognitive score. We will use a 3-tier model for prioritisation, based on the quality of data. This approach has been chosen to minimise loss to follow-up assuming that little data is better than no data at all.
Discussion: Follow-up at the age of 2 years is important for intervention trials in the newborn period as only time can show real benefits and harms later in childhood. To decrease the risk of generalisation and data-driven biased conclusions, we present a detailed description of the methodology for the SafeBoosC-III follow-up study. As funding is limited, a pragmatic approach is necessary.
Trial registration: ClinicalTrials.gov NCT05134116 . Registered on 24 November 2021.
Keywords: Brain injury; Follow-up; Near-infrared spectroscopy; Neurodevelopment; Preterm; Protocol; Randomised clinical trial.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller A-B, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet (British Edition) 2012;379(9832):2162–2172. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
