

Efficacy and safety of radiofrequency ablation for primary and secondary hyperparathyroidism: a retrospective study
- PMID: 37805586
- PMCID: PMC10560222
- DOI: 10.1038/s41598-023-44204-5
Efficacy and safety of radiofrequency ablation for primary and secondary hyperparathyroidism: a retrospective study
Abstract
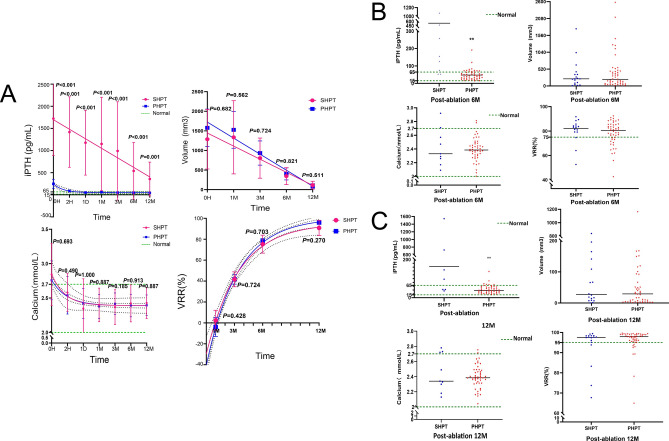
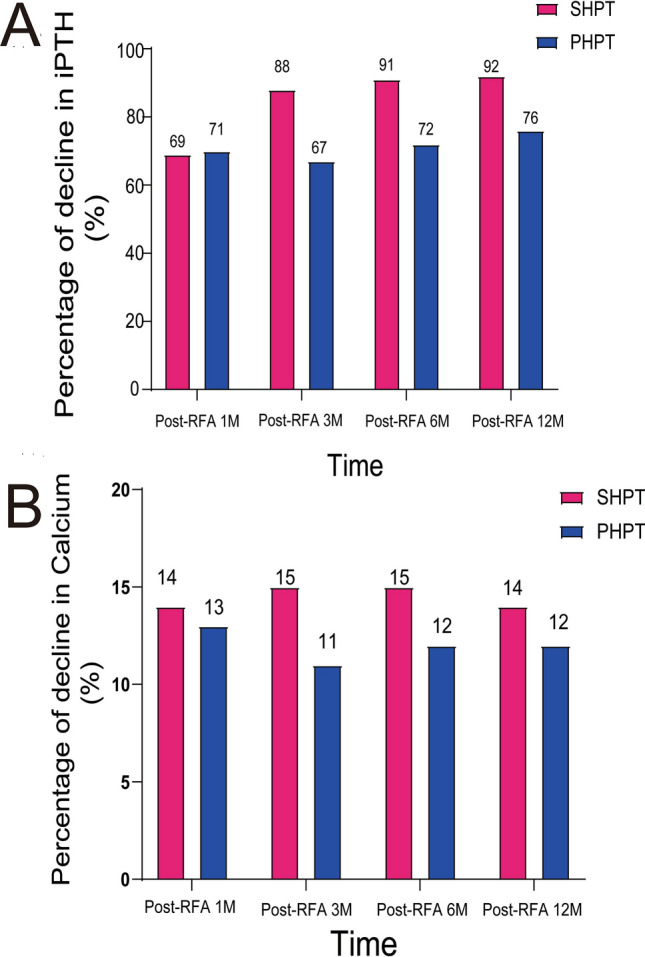
There is now growing interest in the use of Ultrasound-guided radiofrequency ablation (RFA) to treat hyperparathyroidism. But the efficacy and limitations of this treatment have not been described in sufficient detail. Assessing and contrasting the effectiveness and safety of RFA in treating primary hyperparathyroidism (PHPT) and secondary hyperparathyroidism (SHPT). This retrospective study included 57 HPT patients (48 for PHPT and 9 for SHPT) who underwent RFA between January 2017 and April 2021. The serum intact parathyroid hormone (iPTH) and calcium, hyperplastic parathyroid volume, volume reduction rate (VRR) before and after RFA, clinical success rate, symptoms, and complications were analyzed and compared. In SHPT group, bone pain (7/9, 77.8%), skin pruritus (4/9, 44.4%), and multiple hyperplastic parathyroid glands (4/9, 44.4%) were more common compared to the PHPT group. After 12 months of follow-up, the serum iPTH, calcium, and the volume of PHPT and SHPT groups had decreased by more than 60%, 10%, and 90%, respectively (P < 0.05). In the VRR, 13 glands of SHPT (72.2%) and 42 glands of PHPT (87.5%) had achieved the clinical success. In addition, the preoperative and postoperative serum iPTH were higher in the SHPT group than in the PHPT group (P < 0.05). In terms of the serum iPTH and calcium, the PHPT group had substantially higher rates of clinical success, with 42 patients (87.5%) and 46 patients (95.8%) meeting the criteria, respectively compared to 3 patients (33.3%) and 6 patients (66.7%) of SHPT group (P < 0.05). After RFA, the clinical symptoms improved in both groups. The overall incidence of complications (hoarseness and postoperative hematoma) of RFA in the two groups was 10.5% (6/57), and hoarseness (3/9, 33.3%) of SHPT group was more common than PHPT group. All the complications were resolved spontaneously within 12 months after symptomatic treatments. In the treatment of PHPT and SHPT, ultrasound-guided RFA is both successful and safe. PHPT patients have better results in restoring normal iPTH by RFA, and have no considerable difference with the SHPT patients in terms of serum calcium, the volume of the ablation area, and the VRR.
© 2023. Springer Nature Limited.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
