

Outcomes and Management of the SARS-CoV2 Omicron Variant in Recipients of Hematopoietic Cell Transplantation and Chimeric Antigen Receptor T Cell Therapy
- PMID: 37806446
- PMCID: PMC11220618
- DOI: 10.1016/j.jtct.2023.09.027
Outcomes and Management of the SARS-CoV2 Omicron Variant in Recipients of Hematopoietic Cell Transplantation and Chimeric Antigen Receptor T Cell Therapy
Abstract
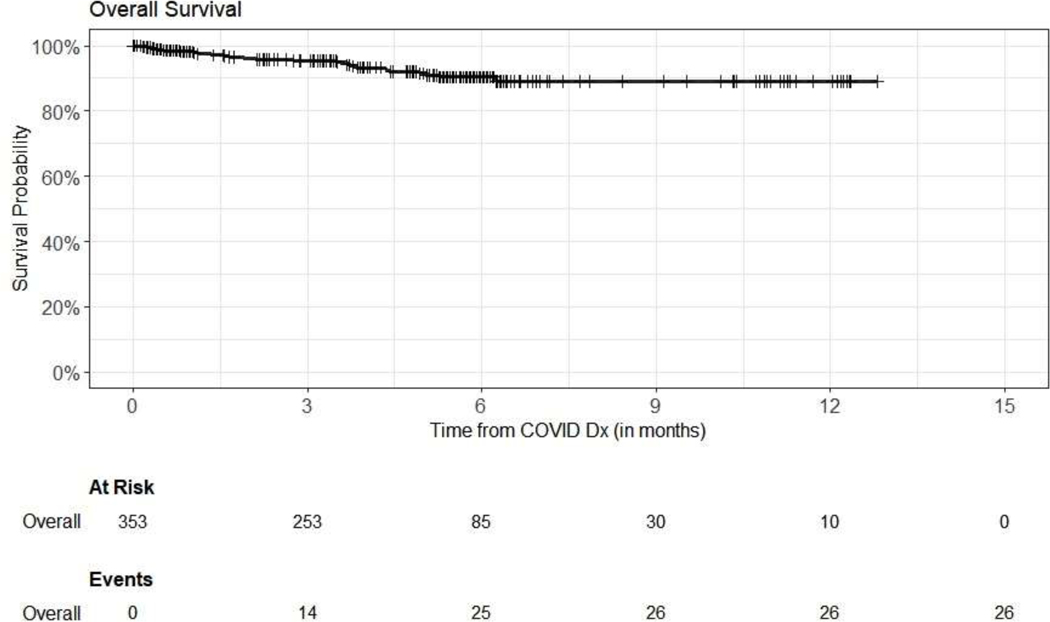
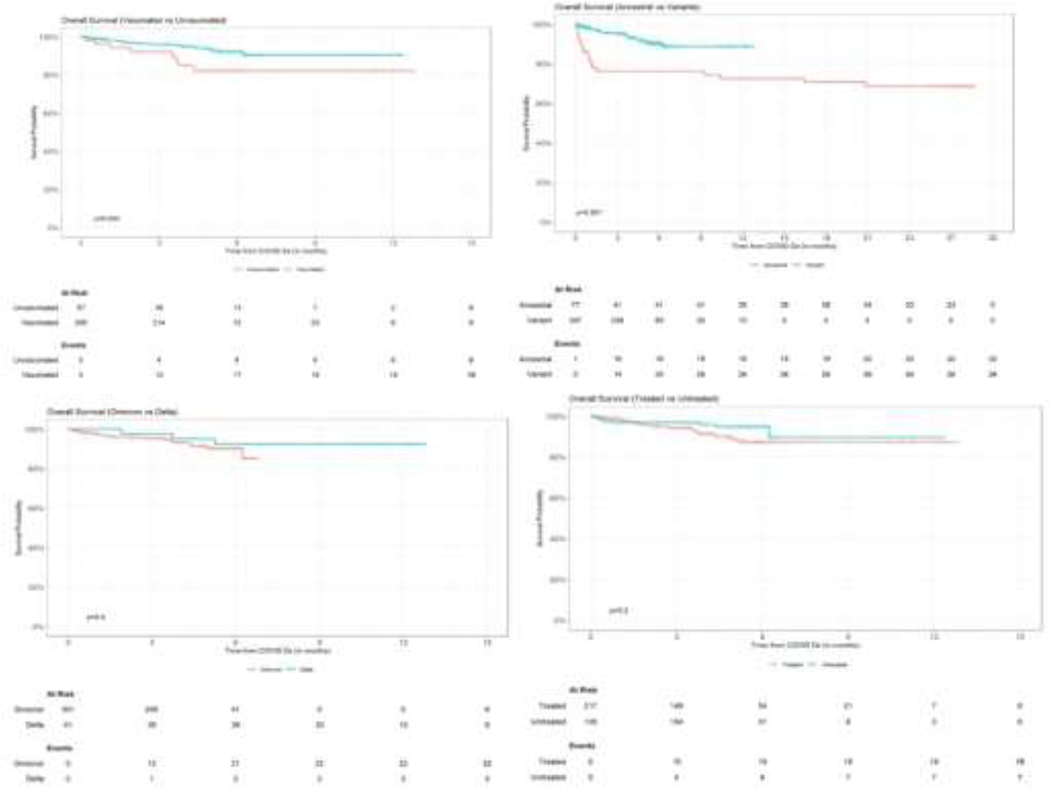
Hematopoietic cell transplantation (HCT) and chimeric antigen receptor T cell therapy (CAR-T) recipients who develop Coronavirus disease 2019 (COVID-19) can have decreased overall survival (OS), likely due to disease-inherent and therapy-related immunodeficiency. The availability of COVID-19-directed therapies and vaccines have improved COVID-19-related outcomes, but immunocompromised individuals remain vulnerable. Specifically, the effects of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variant infections, including Omicron and its sublineages, particularly in HCT recipients, remain to be defined. The aim of this study was to compare the impact of SARS-CoV-2 Omicron infections in HCT/CAR-T recipients with outcomes previously reported for ancestral SARS-CoV-2 infections early in the pandemic (March to June 2020). This was a retrospective analysis of adult HCT/CAR-T recipients diagnosed with COVID-19 at Memorial Sloan Kettering Cancer Center between July 2021 and July 2022. We identified 353 patients (172 autologous HCT recipients [49%], 152 allogeneic HCT recipients [43%], and 29 CAR-T recipients [8%]), with a median time from HCT/CAR-T to SARS-CoV-2 infection of 1010 days (interquartile range, 300 to 2046 days). Forty-one patients (12%) were diagnosed with COVID-19 during the delta wave, and 312 patients (88%) were diagnosed during the Omicron wave. Risk factors associated with increased odds of COVID-19-related hospitalization were the presence of 2 or more comorbidities (odds ratio [OR], 4.9; 95% confidence interval [CI], 2.4 to 10.7; P < .001), CAR-T therapy compared to allogeneic HCT (OR, 7.7; 95% CI, 3.0 to 20.0; P < .001), hypogammaglobulinemia (OR, 2.71; 95% CI, 1.06 to 6.40; P = .027), and age at COVID-19 diagnosis (OR, 1.03; 95% CI, 1.0 to 1.05; P = .04). In contrast, infection during the Omicron variant BA5/BA4-dominant period compared to variant BA1 (OR, .21; 95% CI, .03 to .73; P = .037) and more than 3 years from HCT/CAR-T therapy to COVID-19 diagnosis compared to early infection at <100 days (OR, .31; 95% CI, .12 to .79; P = .011) were associated with a decreased odds for hospitalization. The OS at 12 months from COVID-19 diagnosis was 89% (95% CI, 84% to 94%), with 6 of 26 deaths attributable to COVID-19. Patients with the ancestral strain of SAR-CoV-2 had a lower OS at 12 months, with 73% (95% CI, 62% to 84%) versus 89% (95% CI, 84% to 94%; P < .001) in the Omicron cohort. Specific COVID-19 treatment was administered in 62% of patients, and 84% were vaccinated with mRNA COVID-19 vaccines. Vaccinated patients had significantly better OS than unvaccinated patients (90% [95% CI, 86% to 95%] versus 82% [95% CI, 72% to 94%] at 12 months; P = .003). No significant difference in OS was observed in patients infected with the Omicron and those infected with the Delta variant (P = .4) or treated with specific COVID-19 treatments compared with those not treated (P = .2). We observed higher OS in HCT and CAR-T recipients infected with the Omicron variants compared to those infected with the ancestral strain of SARS-CoV2. The use of COVID-19 antivirals, mAbs, and vaccines might have contributed to the improved outcomes.
Keywords: COVID-19 infection; COVID-19 therapy; HCT and CAR-T patients; Serologic response; Vaccination.
Copyright © 2023 The American Society for Transplantation and Cellular Therapy. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The rest of the authors declare no COIs.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
