

Extra-anatomical left common carotid and subclavian artery bypass followed by aortic arch replacement with frozen elephant trunk
- PMID: 37807044
- PMCID: PMC10561458
- DOI: 10.1186/s13019-023-02403-1
Extra-anatomical left common carotid and subclavian artery bypass followed by aortic arch replacement with frozen elephant trunk
Abstract
Background: Total arch replacement (TAR) using a frozen elephant trunk (FET) allows for simultaneous treatment of the aortic arch and descending aortic pathology via median sternotomy. In addition, an extra-anatomical bypass performed between the left common carotid artery (CCA) and subclavian artery (SCA) prior to TAR allowed further proximalisation of the FET prosthesis, facilitated distal anastomosis of the TAR and spared the demanding left subclavian artery (LSA) anastomosis in the deep thorax. We investigated the efficacy of this debranching-first technique, followed by TAR using a frozen elephant trunk, as a two-stage operation for extensive thoracic aortic aneurysms in high-risk patients.
Methods: Forty-nine consecutive patients with diffuse degenerative aneurysms from the aortic arch to the descending aorta or chronic aortic dissection who underwent left common carotid to subclavian artery bypass followed by TAR using a frozen elephant trunk and subsequent thoracic endovascular aortic repair between 2016 and 2021 were analysed. The baseline characteristics and clinical outcomes were assessed. The estimated overall survival, 5-year aortic event-free survival, and aortic reintervention rates were analysed.
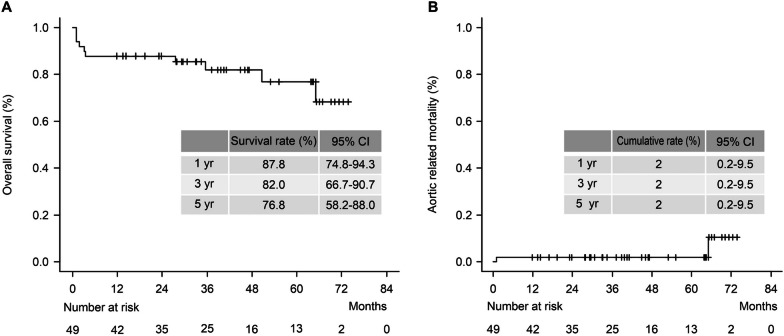
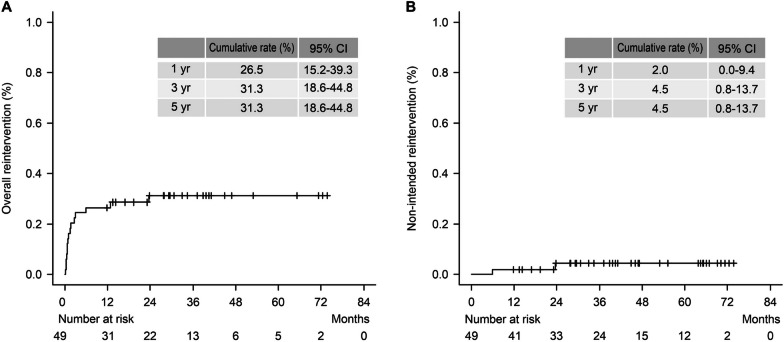
Results: The average European System for Cardiac Operative Risk Evaluation (EuroSCORE II) was 4.7 ± 2.5. The operative mortality rate was 4.1%, with no paraplegia events. The estimated 5-year overall survival, cumulative aortic-related mortality rates were 76.8% and 2%, respectively. The estimated 5-year overall cumulative aortic reintervention rate, including the intended intervention, was 31.3%. The estimated 5-year cumulative rate of non-intended reintervention was 4.5%.
Conclusions: The assessed technique enables a less technically demanding surgery with reasonable outcomes. The estimated 5-year aortic event-free survival and reintervention rates were acceptable, suggesting that multiple stages of alternative open and endovascular interventions, such as this technique, may reduce the morbidity and mortality rates of high-risk patients with diffuse thoracic aortic aneurysm. UMIN-CTR (University hospital Medical Information Network-Clinical Trial Registry) https://center6.umin.ac.jp/cgi-open-bin/ctr_e/index.cgi Clinical registration number: UMIN000051531.
Keywords: Debranching-first technique; Frozen elephant trunk; Total arch replacement.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
We have no conflicts of interest to disclose.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
