

Predictors of outcomes in patients with obesity following mitral valve surgery
- PMID: 37808032
- PMCID: PMC10556846
- DOI: 10.1016/j.xjon.2023.03.017
Predictors of outcomes in patients with obesity following mitral valve surgery
Abstract
Objective: Few studies have assessed the outcomes of mitral valve surgery in patients with obesity. We sought to study factors that determine the in-hospital outcomes of this population to help clinicians provide optimal care.
Methods: A retrospective analysis of adult patients with obesity who underwent open mitral valve replacement or repair between January 1, 2012, and December 31, 2020, was conducted using the National Inpatient Sample. Weighted logistic regression and random forest analyses were performed to assess factors associated with mortality and the interaction of each variable.
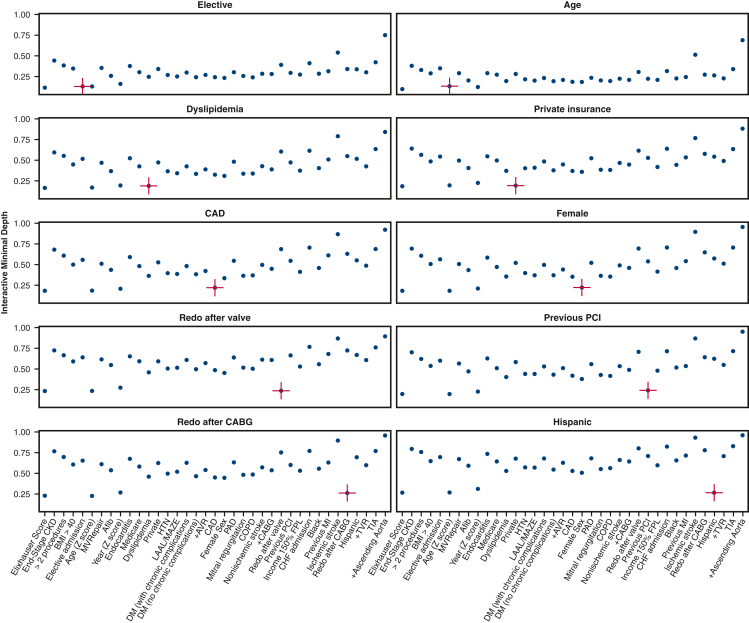
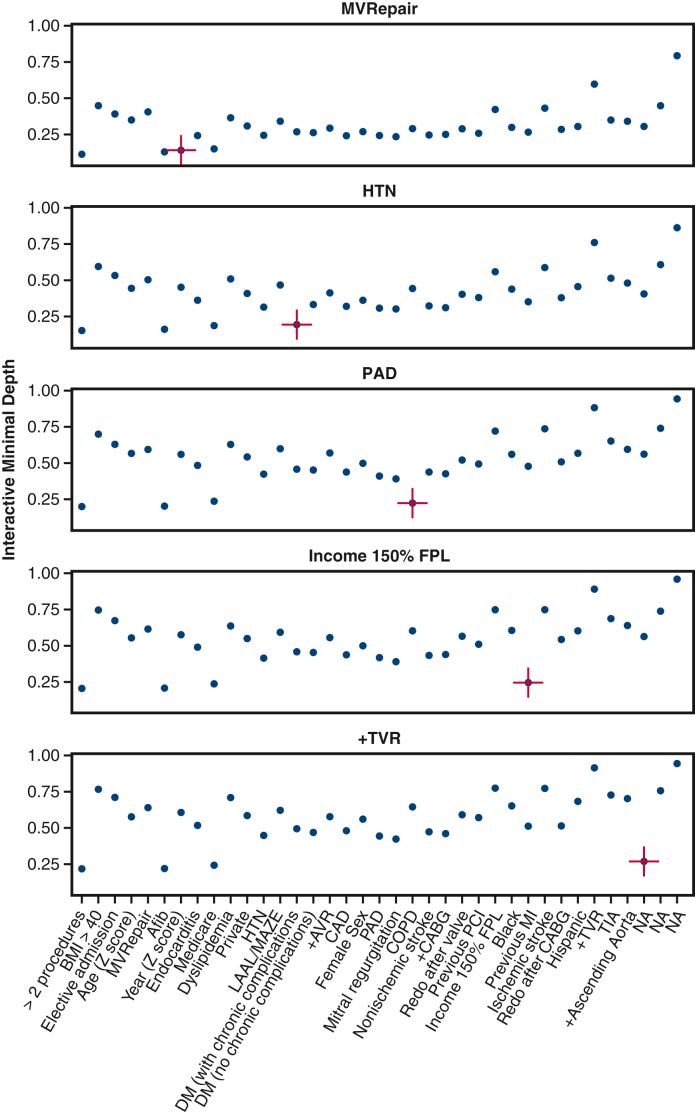
Results: Of the 48,775 patients with obesity, 34% had morbid obesity (body mass index ≥40), 55% were women, 66% underwent elective surgery, and 55% received isolated open mitral valve replacement or repair. In-hospital mortality was 5.0% (n = 2430). After adjusting for important covariates, a greater risk of mortality was associated with older patients (adjusted odds ratio [aOR], 1.24; 95% CI, 1.08-1.43), higher Elixhauser comorbidity score (aOR, 2.10; 95% CI, 1.87-2.36), prior valve surgery (aOR, 1.63; 95% CI, 1.01-2.63), and more than 2 concomitant procedures (aOR, 2.83; 95% CI, 2.07-3.85). Lower mortality was associated with elective admissions (aOR, 0.70; 95% CI, 0.56-0.87) and valve repair (aOR, 0.58; 95% CI, 0.46-0.73). Machine learning identified several interactions associated with early mortality, such as Elixhauser score, female sex, body mass index ≥40, and kidney failure.
Conclusions: The complexity of presentation, comorbidities in older and female patients, and morbid obesity are independently associated with an increased risk of mortality in patients undergoing open mitral valve replacement or repair. Morbid obesity and sex disparity should be recognized in this population, and physicians should consider older patients and females with multiple comorbidities for earlier and more opportune treatment windows.
Keywords: adult cardiac; machine learning; mitral valve; mortality; obesity; random forest.
© 2023 The Author(s).
Figures










References
-
- Lavie C.J., Arena R., Alpert M.A., Milani R.V., Ventura H.O. Management of cardiovascular diseases in patients with obesity. Nat Rev Cardiol. 2018;15:45–56. - PubMed
-
- Habib R.H., Zacharias A., Schwann T.A., Riordan C.J., Durham S.J., Shah A. Effects of obesity and small body size on operative and long-term outcomes of coronary artery bypass surgery: a propensity-matched analysis. Ann Thorac Surg. 2005;79:1976–1986. - PubMed
-
- Benjamin E.J., Muntner P., Alonso A., Bittencourt M.S., Callaway C.W., Carson A.P., et al. Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation. 2019;139:e56–e528. - PubMed
E-References
-
- Lumley C.T. Survey: Analysis of Complex Survey Samples. R Package Version 4.0. https://cran.r-project.org/package=survey
-
- Gasparini A. Comorbidity: an R package for computing comorbidity scores. J Open Source Softw. 2018;3:648.
-
- Mayer M. missRanger: fast imputation of missing values. R package version 2.1.3. 2021. https://CRAN.R-project.org/package=missRanger
-
- Ishwaran H., Lu M., Kogalur U.B. randomForestSRC: getting started with randomForestSRC vignette. 2021. http://randomforestsrc.org/articles/getstarted.html
-
- Ishwaran H., Lu M., Kogalur U.B. randomForestSRC: variable importance (VIMP) with subsampling inference vignette. 2021. http://randomforestsrc.org/articles/vimp.html
LinkOut - more resources
Full Text Sources
