

Minimally invasive approach associated with lower resource utilization after aortic and mitral valve surgery
- PMID: 37808048
- PMCID: PMC10556938
- DOI: 10.1016/j.xjon.2023.06.007
Minimally invasive approach associated with lower resource utilization after aortic and mitral valve surgery
Abstract
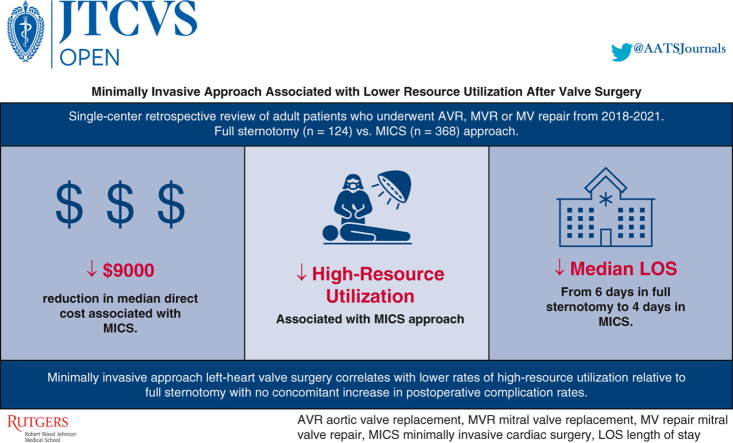
Objective: To investigate the effect of minimally invasive cardiac surgery (MICS) on resource utilization, cost, and postoperative outcomes in patients undergoing left-heart valve operations.
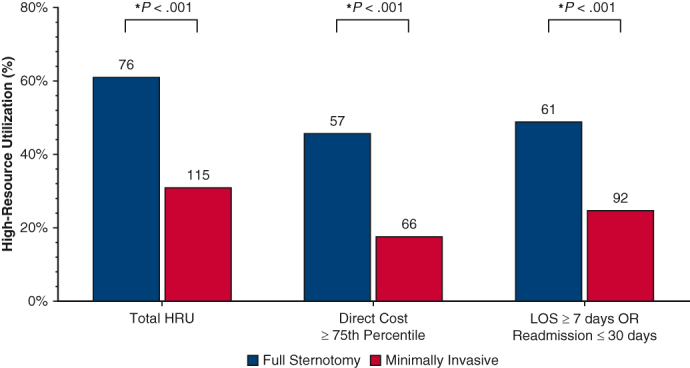
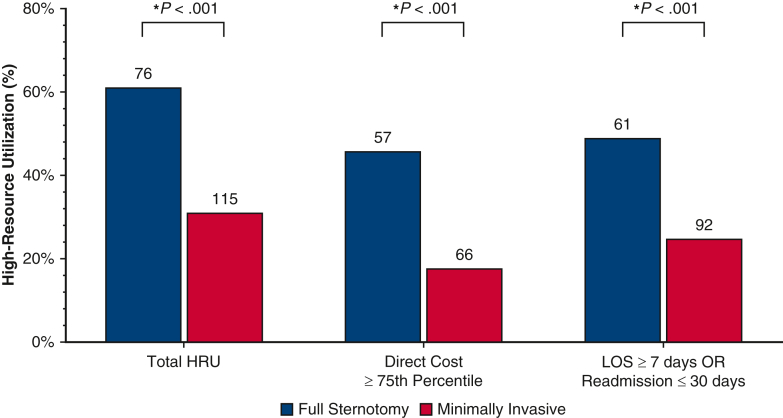
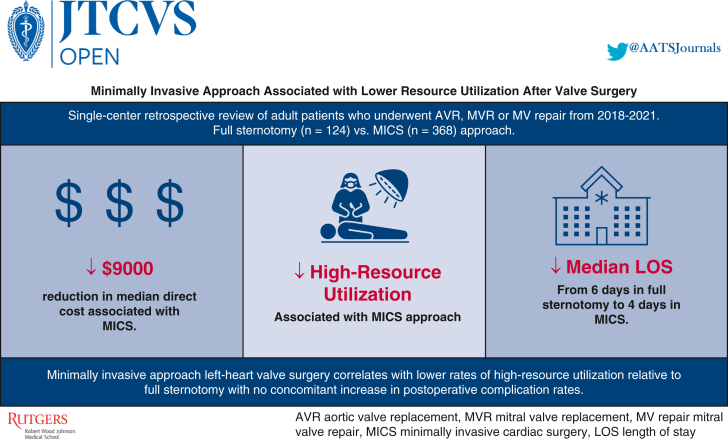
Methods: Data were retrospectively reviewed for patients undergoing single-valve surgery (eg, aortic valve replacement, mitral valve replacement, or mitral valve repair) at a single center from 2018 to 2021, stratified by surgical approach: MICS vs full sternotomy (FS). Baseline characteristics and postoperative outcomes were compared. Primary outcome was high resource utilization, defined as direct procedure cost higher than the third quartile or either postoperative LOS ≥7 days or 30-day readmission. Secondary outcomes were direct cost, length of stay, 30-day readmission, in-hospital and 30-day mortality, and major morbidity. Multiple regression analysis was conducted, controlling for baseline characteristics, operative approach, valve operation, and lead surgeon to assess high resource utilization.
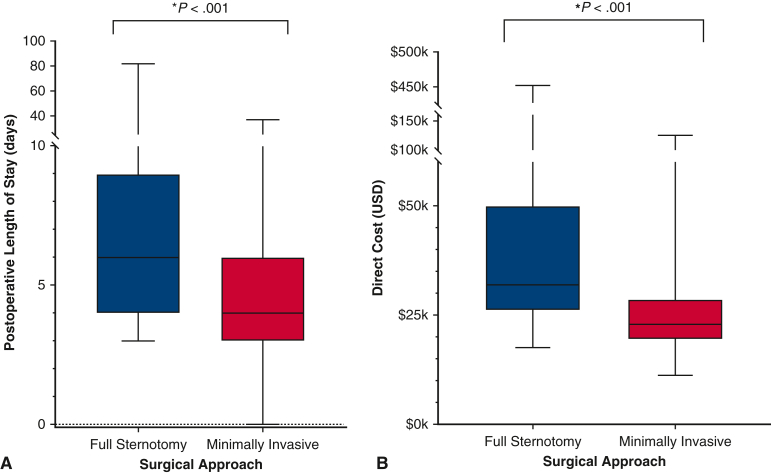
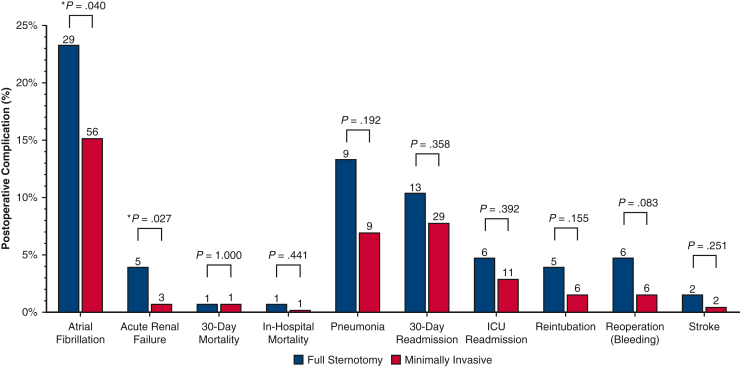
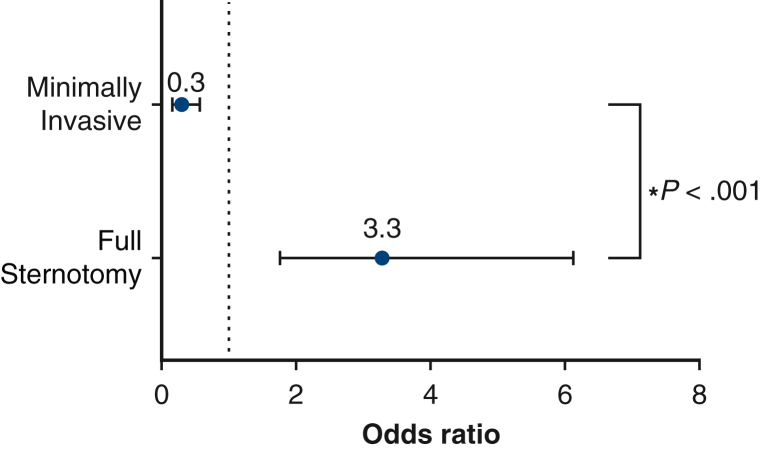
Results: MICS was correlated with a significantly lower rate of high resource utilization (MICS, 31.25% [n = 115] vs FS 61.29% [n = 76]; P < .001). Median postoperative length of stay (MICS, 4 days [range, 3-6 days] vs FS, 6 days [range, 4 to 9 days]; P < .001) and direct cost (MICS, $22,900 [$19,500-$28,600] vs FS, $31,900 [$25,900-$50,000]; P < .001) were lower in the MICS group. FS patients were more likely to experience postoperative atrial fibrillation (P = .040) and renal failure (P = .027). Other outcomes did not differ between groups. Controlling for stratified Society of Thoracic Surgeons predicted risk of mortality, cardiac valve operation, and lead surgeon, FS demonstrated increased likelihood of high resource utilization (P < .001).
Conclusions: MICS for left-heart valve pathology demonstrated improved postoperative outcomes and resource utilization.
Keywords: high-resource utilization; left heart valve surgery; minimally-invasive surgery.
© 2023 The Author(s).
Figures

References
-
- Lim J.Y., Deo S.V., Altarabsheh S.E., Jung S.H., Erwin P.J., Markowitz A.H., et al. Conventional versus minimally invasive aortic valve replacement: pooled analysis of propensity-matched data. J Card Surg. 2015;30:125–134. - PubMed
LinkOut - more resources
Full Text Sources
