

Loop Excision for Precancers of the Uterine Cervix: Local or General Anaesthetic?
- PMID: 37808260
- PMCID: PMC10556877
- DOI: 10.1055/a-2150-0835
Loop Excision for Precancers of the Uterine Cervix: Local or General Anaesthetic?
Abstract
Aim: In Germany, treatment of HSIL or AIS of the uterine cervix by loop excision is performed almost exclusively under general anaesthesia (GA). International studies and guidelines show high acceptance of local anaesthesia (LA) due to hermeneutic, medical, and economic factors. We performed an observational comparative study aiming to prove advantages of local anaesthesia within the German health system.
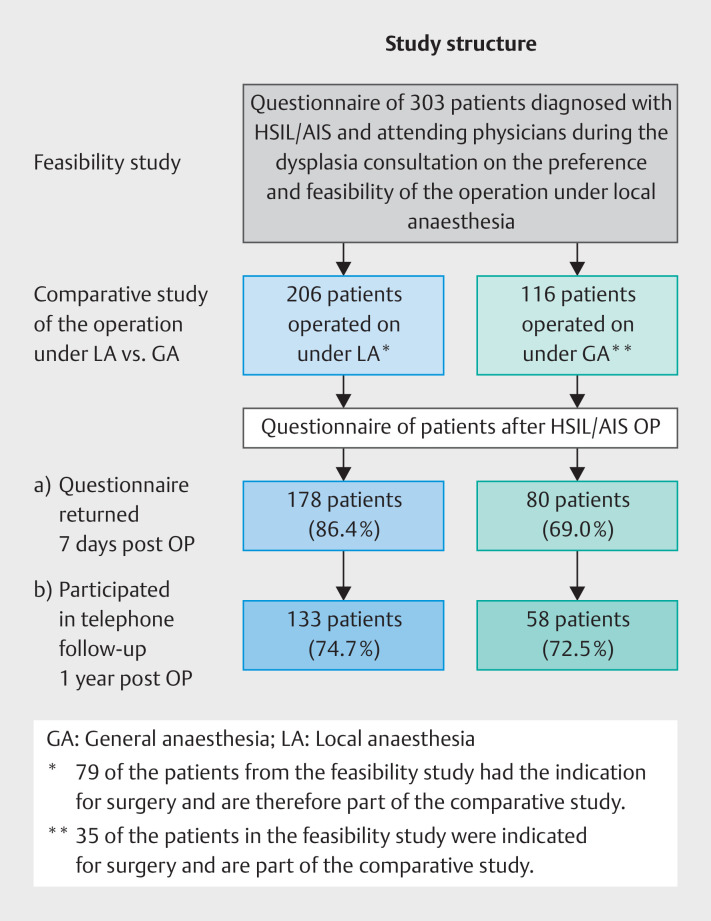
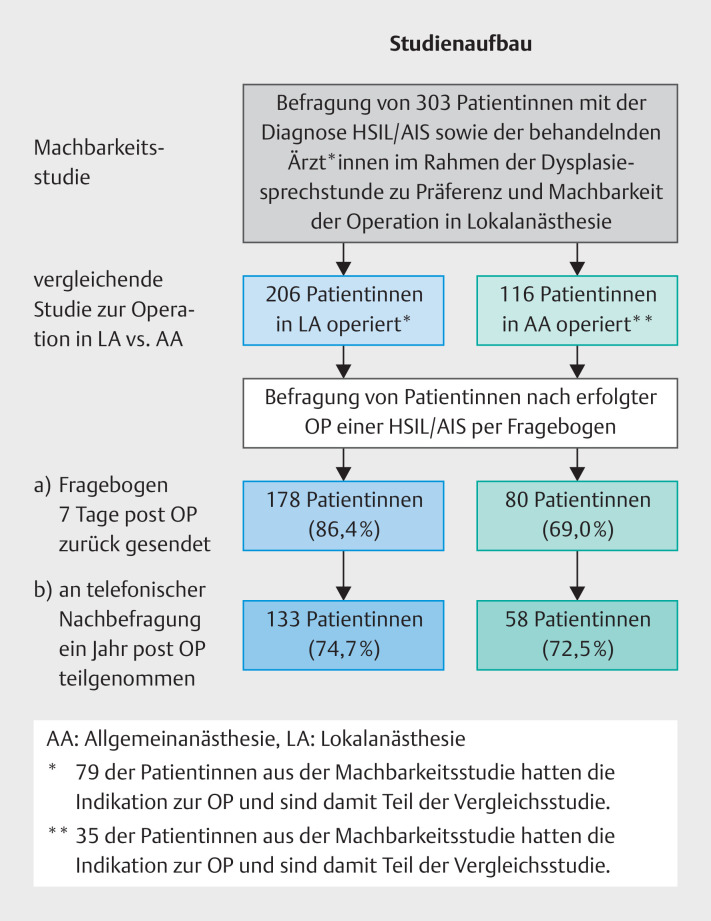
Patients and methods: In a prospective observational study, patients diagnosed with HSIL or AIS of the uterine cervix were treated at the Institute for Cytology and Dysplasia, Berlin, by loop excision in 2021. We started with a feasibility study : 303 patients diagnosed with HSIL/AIS of the uterine cervix and her colposcopist answered an electronic questionnaire with respect to loop excision under LA. Since we found a high acceptance for LA in patients and colposcopists, we initiated a comparative study LA vs. GA: 322 patients underwent loop excision and selected their mode of anaesthesia: n = 206 LA vs. n = 116 GA. 114 patients of the feasibility study had to undergo loop excision and became part of the comparative study (n = 79 for the LA group, n = 35 for the GA group). All patients received a standardised questionnaire to document their pain score within 24 h after treatment on a visual analogue scale, i.e. VAS, between 0 and 100. 178 patients of the LA group and 80 patients of the GA group completed and returned the questionnaire and form the cohort for our comparison of LA vs. GA. With 191 of these 258 patients, i.e. 74%, a telephone survey was performed to ask for patient satisfaction and the rates of recurrence after a mean interval of 1 year post surgery. We postulate that there will be no clinically relevant significant difference in satisfaction and postoperative pain between patients in the LA group and the GA group.
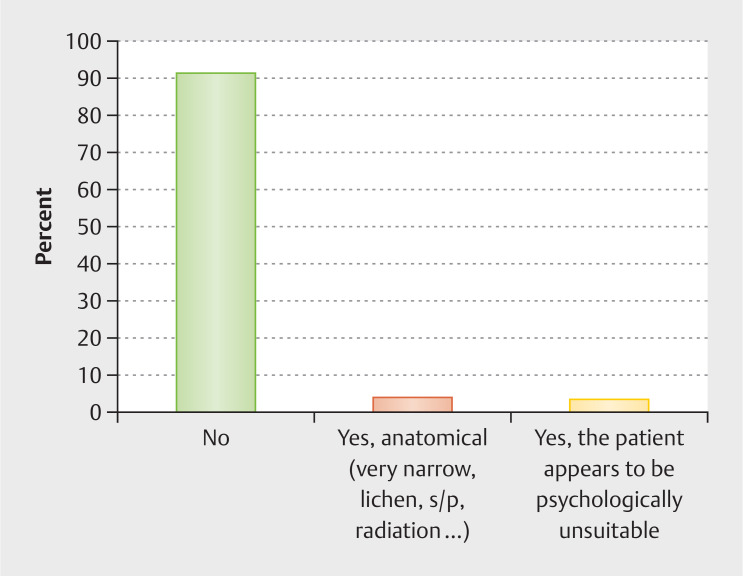
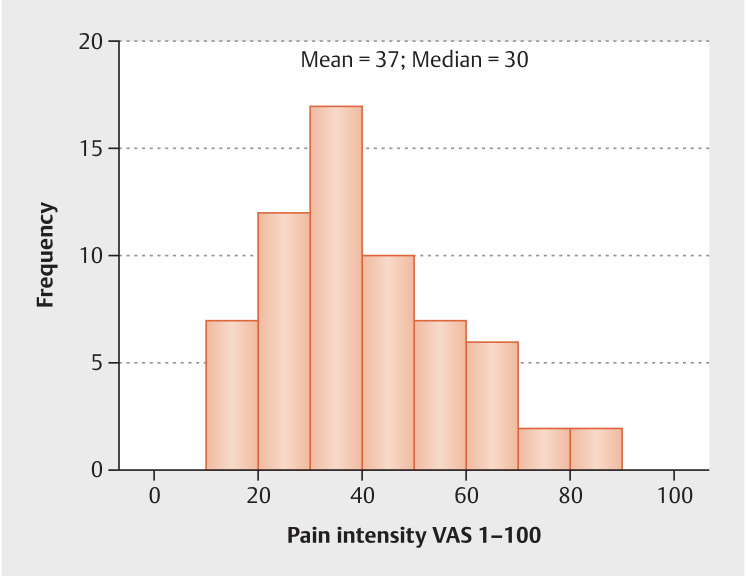
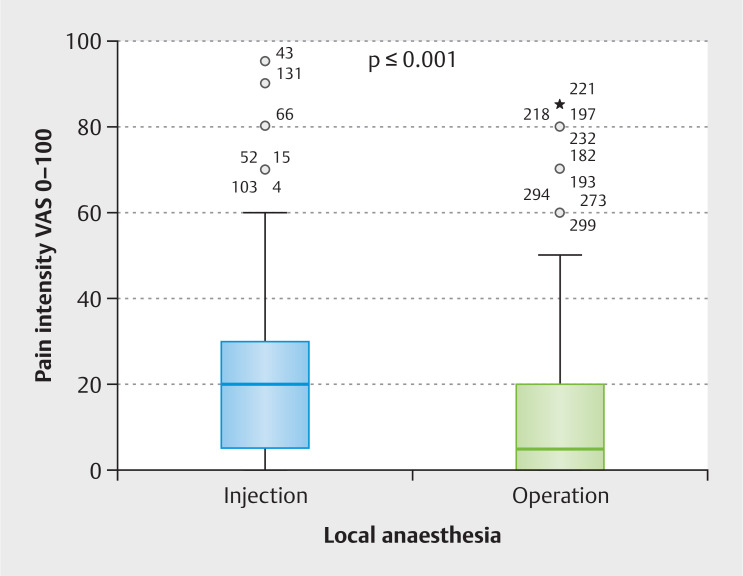
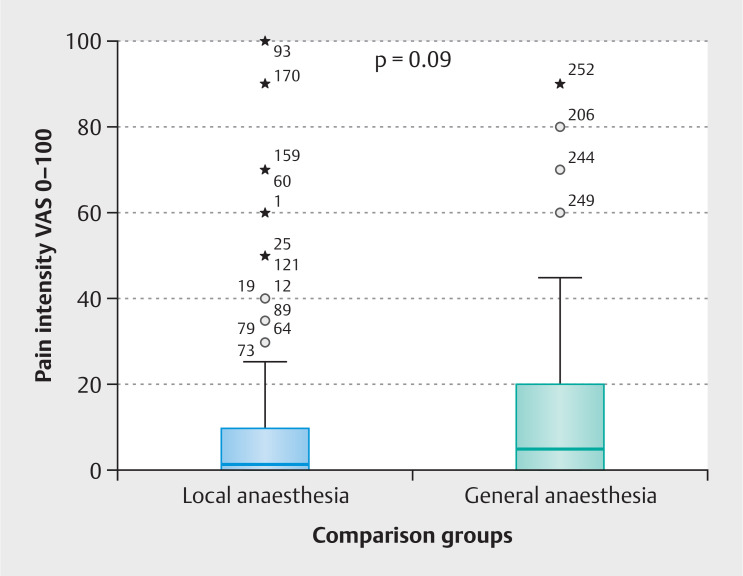
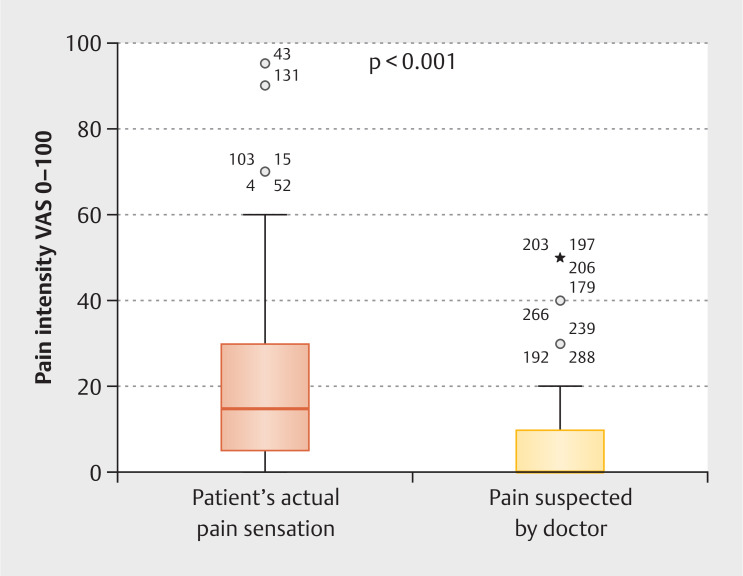
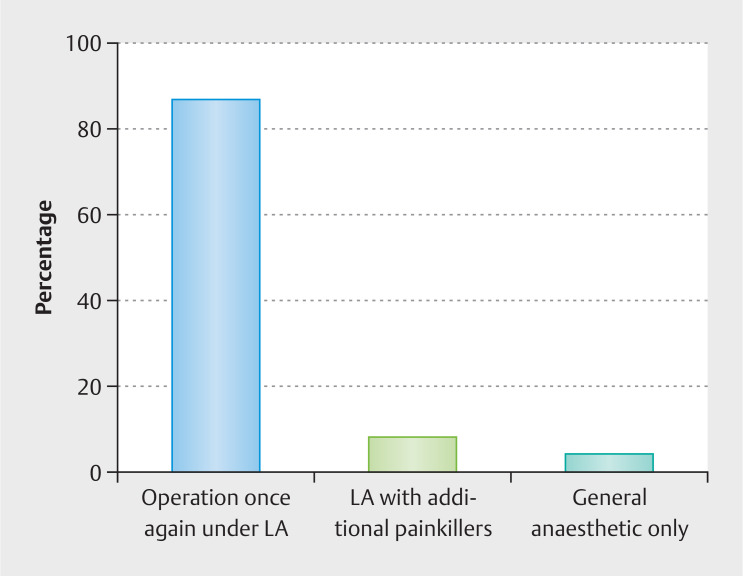
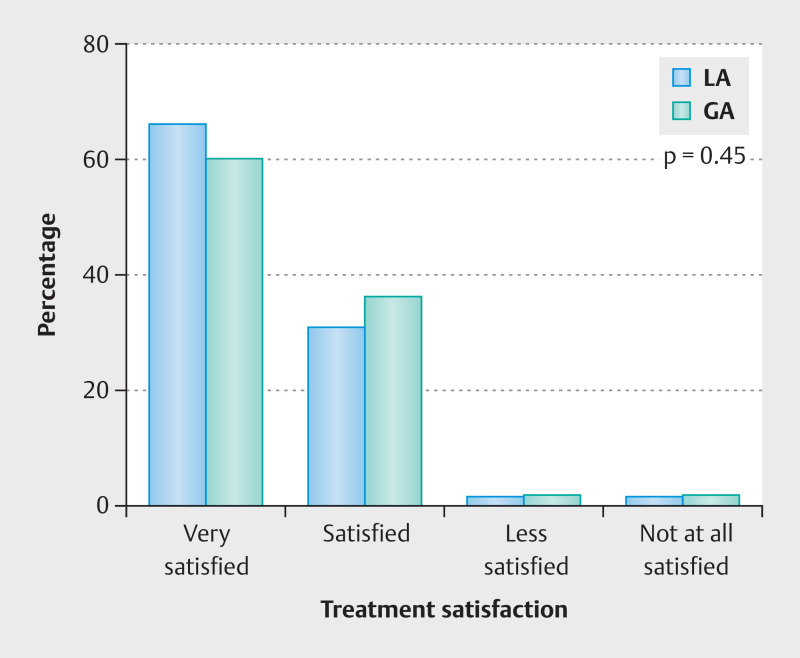
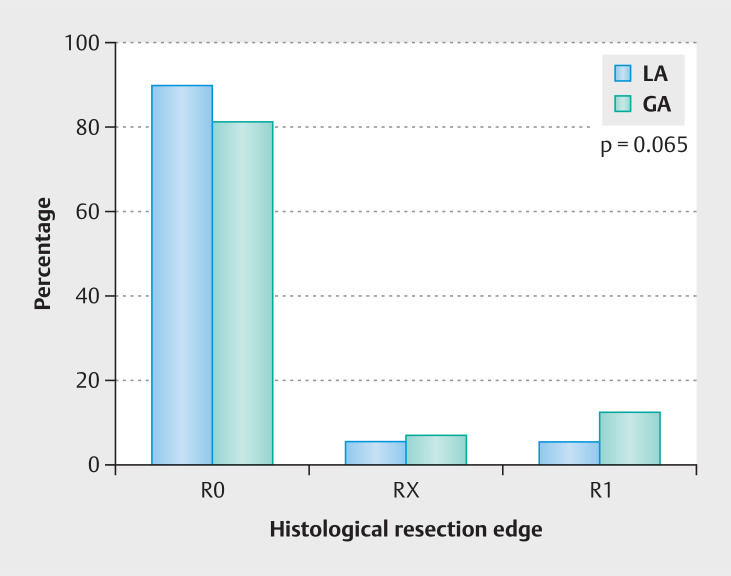
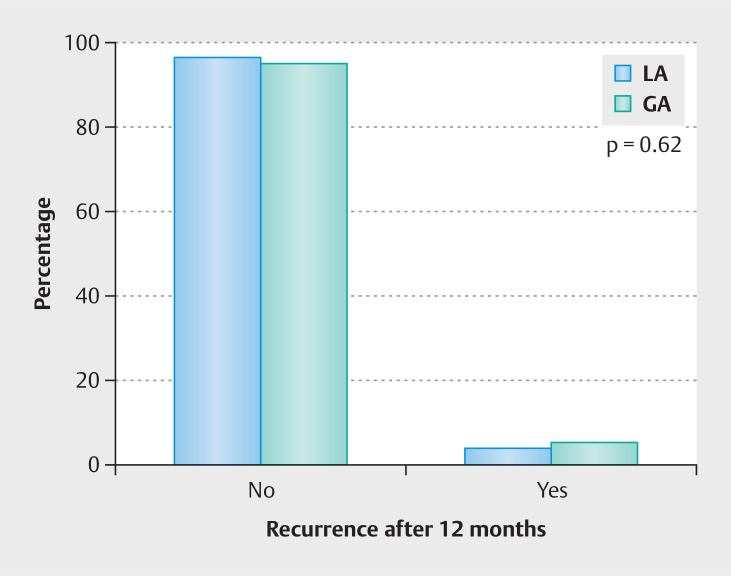
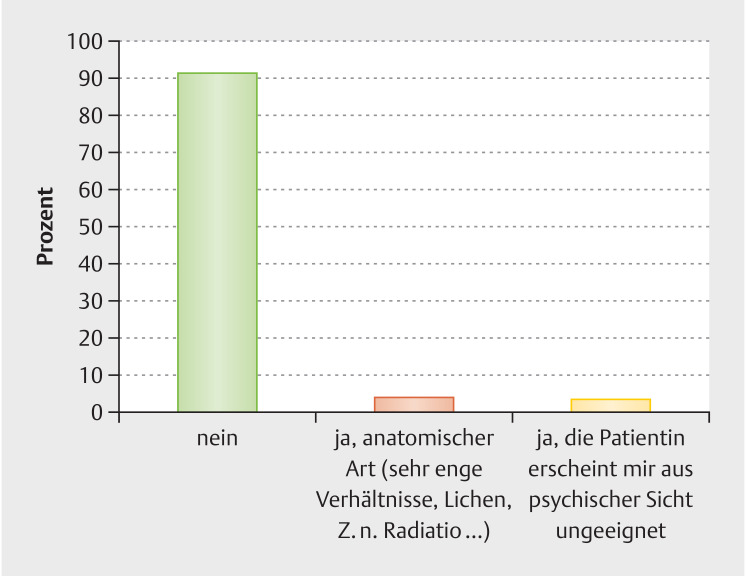
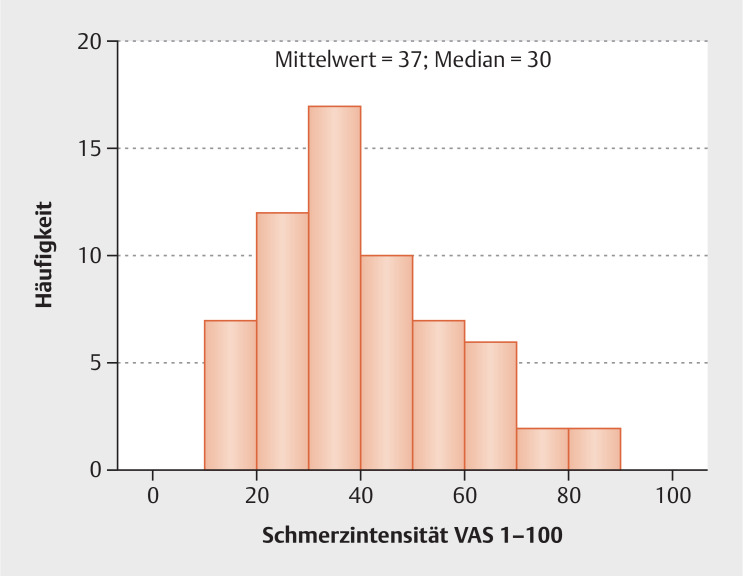
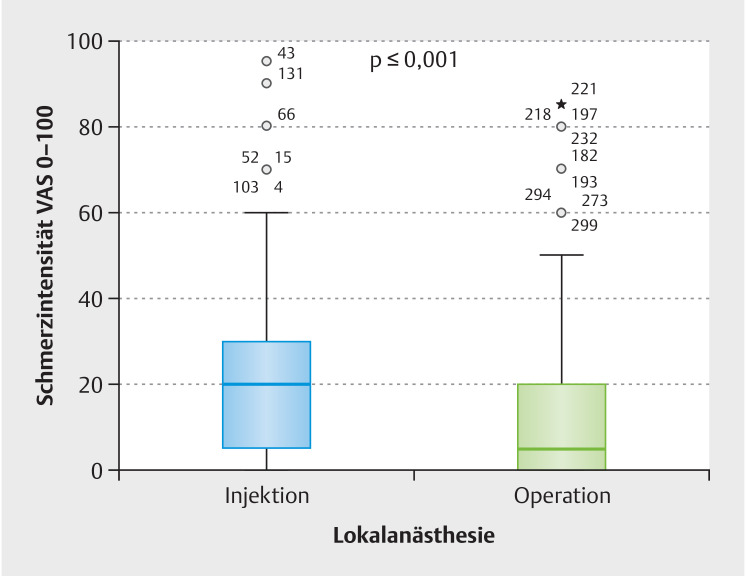
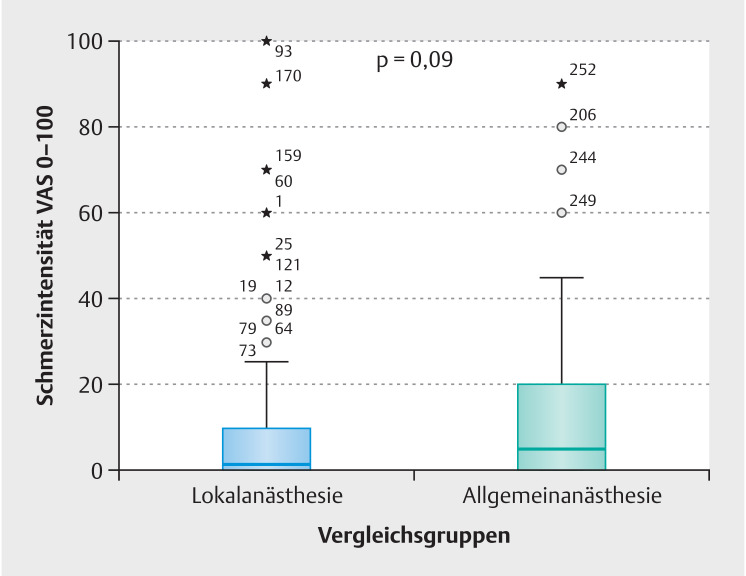
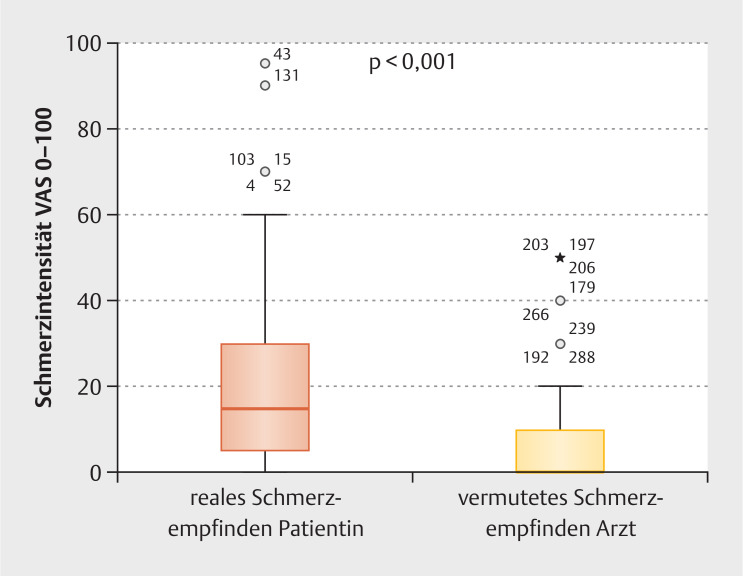
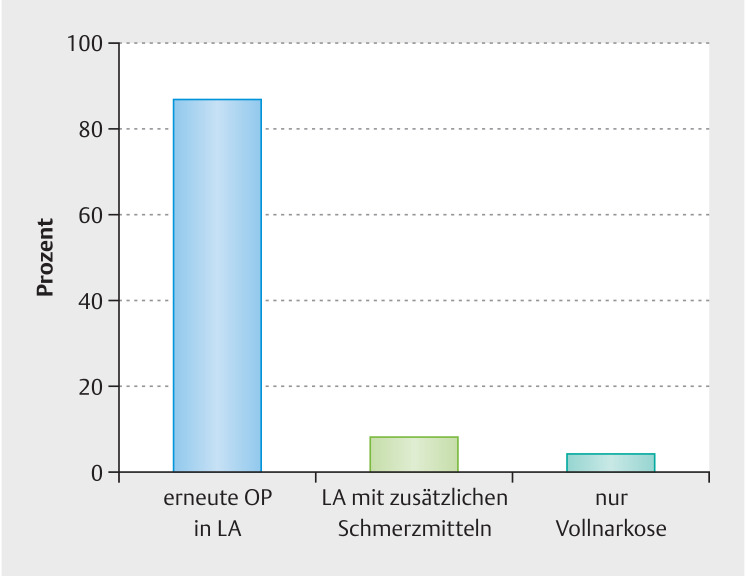
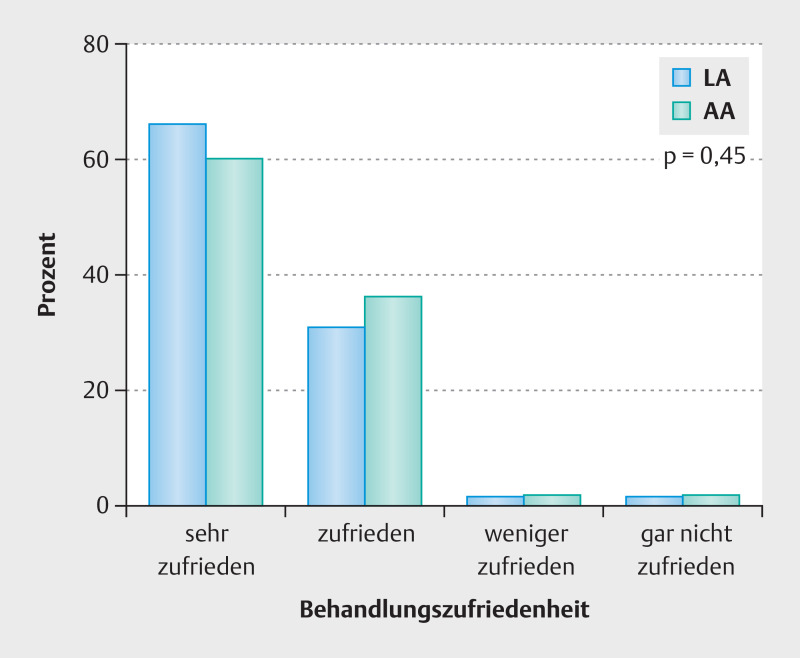
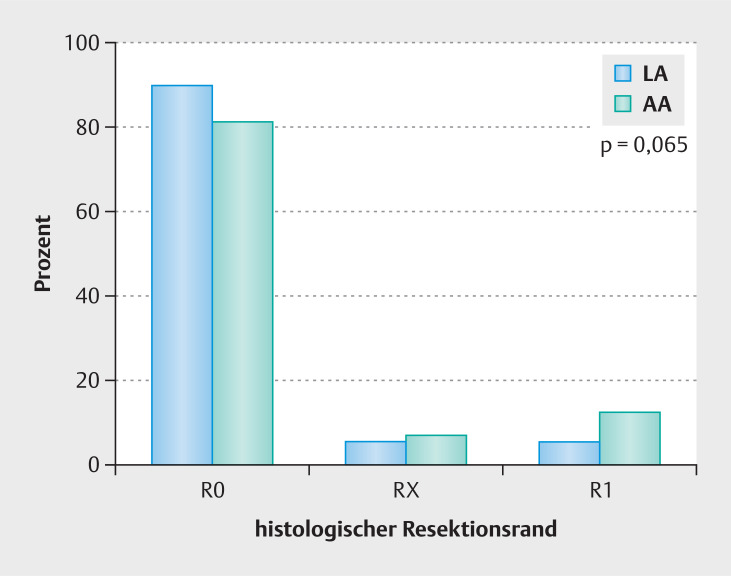
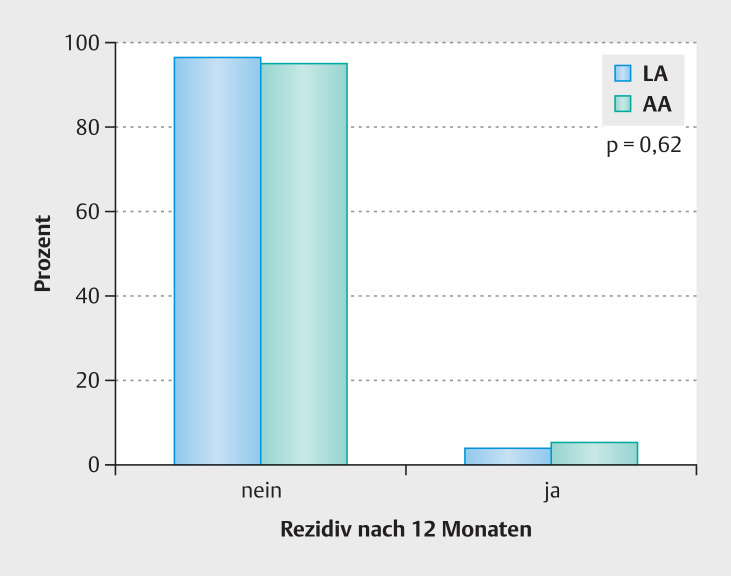
Results: In the feasibility study , 90% (272 of 303) of patients diagnosed with HSIL or AIS were considered eligible for LA by their colposcopists. 75% (227 of 303) of patients were open to loop excision under LA. In the comparative study , 63 of 206 women of the LA group were interviewed preoperatively: 89% would accept a pain score above 20 during the procedure, 33% a pain score above 50 and 11% of max. 20. Postoperatively, the median VAS pain score for loop excision under local anaesthesia was 13.1 in 178 patients, and pain during injection of local anaesthesia was 20.9 (p < 0.001). The VAS pain score 20 minutes post surgery did not differ significantly between 178 patients after local anaesthesia versus 80 patients after general anaesthesia (p = 0.09). The surgeons estimated the patient's pain significantly less than the patients themselves with an underestimate of -14.63 points on the VAS (p < 0.001). Within 7 days following loop excision under LA, 95.5% of 178 patients would choose local anaesthesia as their preferred method for a potential repeat loop excision, 8.8% of which would like additional painkillers, and 4.5% would choose general anaesthesia.In a telephone follow-up survey of 133 women from the LA group after a mean of 12 months post surgery, 97% were "satisfied" or "very satisfied" with the treatment carried out. For patient satisfaction and postoperative pain, no clinically relevant significant difference was seen between the LA and the GA group.The rate of secondary bleeding (6.7% vs. 8.1%, p = 0.72), recurrence of HSIL/AIS (3.6% vs. 5.2%, p = 0.62), and the distribution of the histopathological R status (R0 89.5% vs. 81.1%, p = 0.73; R1 5.3% vs.12.2%, p = 0.57, Rx 4.1% vs. 5.4%, p = 0.65) showed no significant difference when comparing the LA group versus the GA group.
Conclusion: Following loop excision under local anaesthesia, more than 95% of patients would choose this method again for repeat surgery. One year post surgery, 97% of the patients were "satisfied" or "very satisfied" with the treatment under local anaesthesia. Offering local anaesthesia for loop excision to patients should be mandatory and included in current guidelines.
Keywords: CIN; Loop excision; local anaesthesia.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial-License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. (https://creativecommons.org/licenses/by-nc-nd/4.0/).
Conflict of interest statement
Conflict of Interest The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Syringe or mask? Loop electrosurgical excision procedure under local or general anesthesia: a randomized trial.Am J Obstet Gynecol. 2020 Dec;223(6):888.e1-888.e9. doi: 10.1016/j.ajog.2020.06.041. Epub 2020 Jul 24. Am J Obstet Gynecol. 2020. PMID: 32585223 Clinical Trial.
-
LLETZ make it simple: Anxiety, pain and treatment outcomes with outpatient large loop excision of the transformation zone under local anaesthesia.Aust N Z J Obstet Gynaecol. 2020 Jun;60(3):438-443. doi: 10.1111/ajo.13121. Epub 2020 Jan 30. Aust N Z J Obstet Gynaecol. 2020. PMID: 32002985
-
Is knee arthroscopy under local anaesthetic a patient-friendly technique? A prospective controlled trial.Eur J Orthop Surg Traumatol. 2016 Aug;26(6):633-8. doi: 10.1007/s00590-016-1799-2. Epub 2016 Jun 21. Eur J Orthop Surg Traumatol. 2016. PMID: 27324262
-
Perioperative local anaesthesia for reducing pain following septal surgery.Cochrane Database Syst Rev. 2018 Aug 23;8(8):CD012047. doi: 10.1002/14651858.CD012047.pub2. Cochrane Database Syst Rev. 2018. PMID: 30136717 Free PMC article.
-
Paravertebral anaesthesia with or without sedation versus general anaesthesia for women undergoing breast cancer surgery.Cochrane Database Syst Rev. 2021 Feb 25;2(2):CD012968. doi: 10.1002/14651858.CD012968.pub2. Cochrane Database Syst Rev. 2021. PMID: 33629404 Free PMC article.
References
LinkOut - more resources
Full Text Sources