

This is a preprint.
Hematologic setpoints are a stable and patient-specific deep phenotype
- PMID: 37808854
- PMCID: PMC10557837
- DOI: 10.1101/2023.09.26.23296146
Hematologic setpoints are a stable and patient-specific deep phenotype
Update in
-
Haematological setpoints are a stable and patient-specific deep phenotype.Nature. 2025 Jan;637(8045):430-438. doi: 10.1038/s41586-024-08264-5. Epub 2024 Dec 11. Nature. 2025. PMID: 39663453 Free PMC article.
Abstract
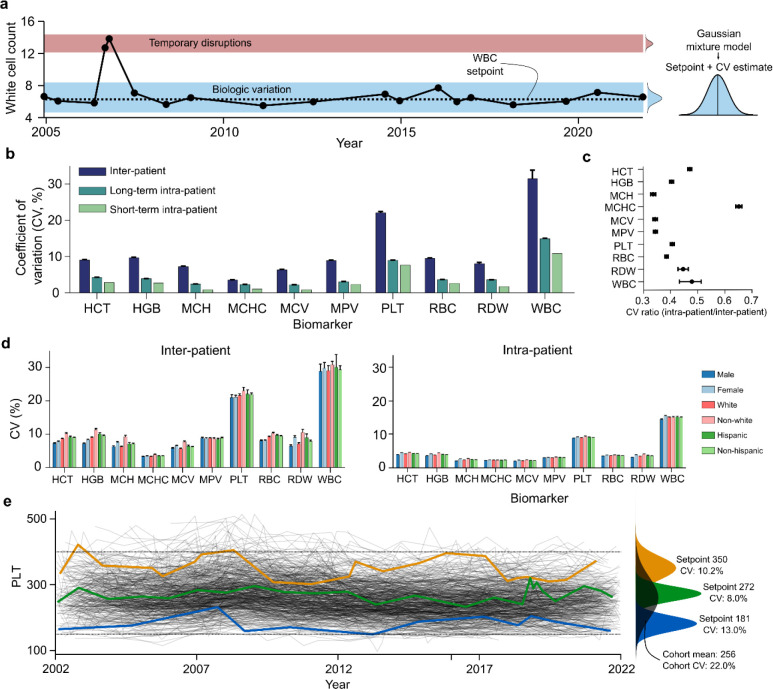
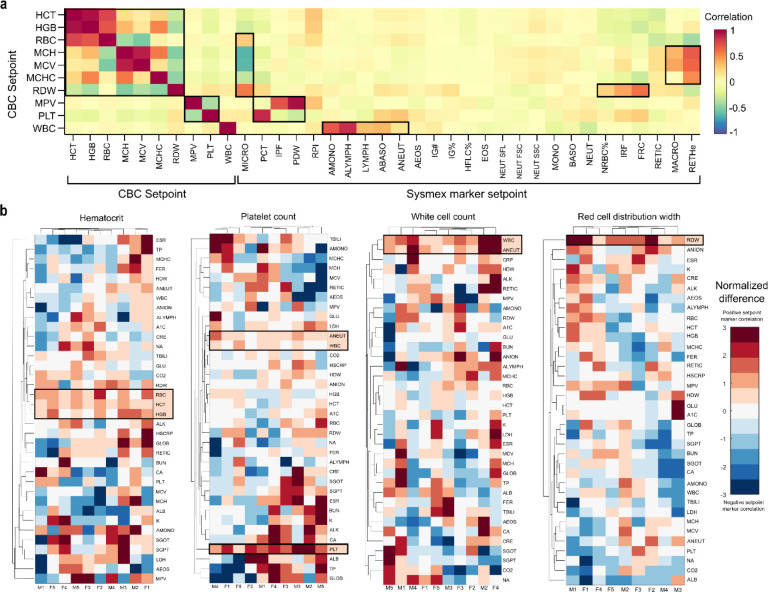
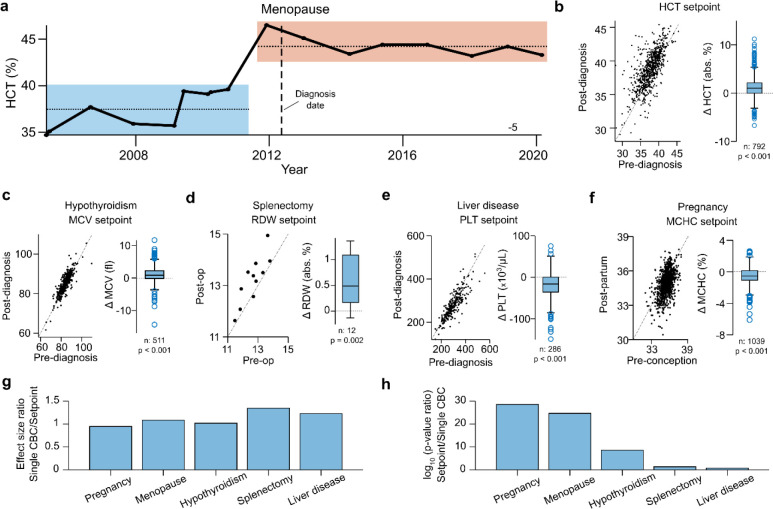
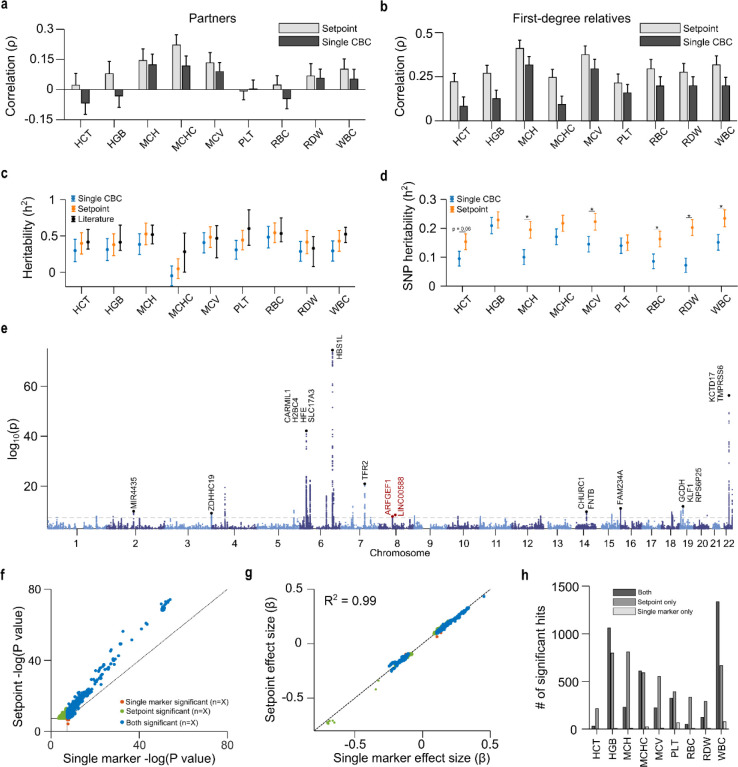
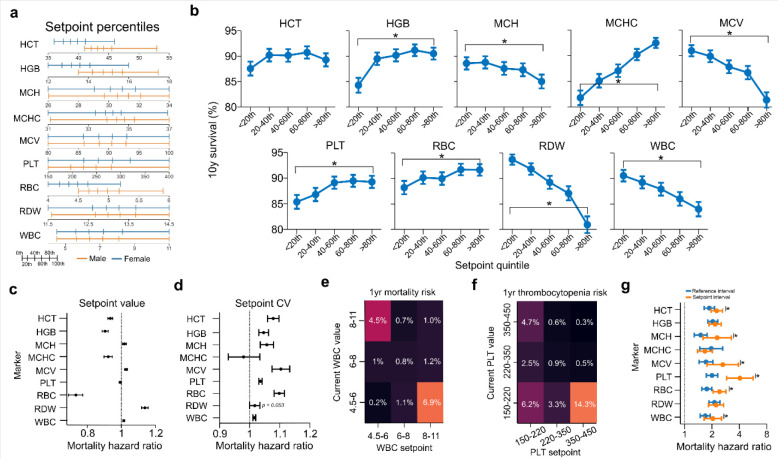
The complete blood count is an important screening tool for healthy adults and is the most commonly ordered test at periodic physical exams. However, results are usually interpreted relative to one-size-fits-all reference intervals, undermining the goal of precision medicine to tailor medical care to the needs of individual patients based on their unique characteristics. Here we show that standard complete blood count indices in healthy adults have robust homeostatic setpoints that are patient-specific and stable, with the typical healthy adult's set of 9 blood count setpoints distinguishable from 98% of others, and with these differences persisting for decades. These setpoints reflect a deep physiologic phenotype, enabling improved detection of both acquired and genetic determinants of hematologic regulation, including discovery of multiple novel loci via GWAS analyses. Patient-specific reference intervals derived from setpoints enable more accurate personalized risk assessment, and the setpoints themselves are significantly correlated with mortality risk, providing new opportunities to enhance patient-specific screening and early intervention. This study shows complete blood count setpoints are sufficiently stable and patient-specific to help realize the promise of precision medicine for healthy adults.
Conflict of interest statement
JMH reports funding from the National Institutes of Health (grant IDs: R01HD104756; R01DK123330). All authors report no conflicts of interest.
Figures
References
-
- Blood Tests - Blood Tests | NHLBI, NIH. Published March 24, 2022. Accessed July 18, 2023. https://www.nhlbi.nih.gov/health/blood-tests
-
- Aarsand A, Fernandez-Calle P, Webster C, et al. The EFLM Biological Variation Database. Accessed February 14, 2023. https://biologicalvariation.eu/
-
- Garner C, Tatu T, Reittie JE, et al. Genetic influences on F cells and other hematologic variables: a twin heritability study. Blood. 2000;95(1):342–346. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources