

Urgent and emergent repair of complex aortic aneurysms using an off-the-shelf branched device
- PMID: 37808886
- PMCID: PMC10556233
- DOI: 10.3389/fcvm.2023.1277459
Urgent and emergent repair of complex aortic aneurysms using an off-the-shelf branched device
Abstract
Introduction: Endovascular repair using off-the-shelf endografts is a viable solution in patients with ruptured or symptomatic complex aortic aneurysms. This analysis aimed to present the peri-operative and follow-up outcomes in urgent and emergent cases managed with the t-Branch multibranched thoracoabdominal endograft.
Methods: Prospectively collected data from all consecutive urgent and emergent cases managed in two aortic centers between January 1st, 2014, to November 30th, 2022, using the t-Branch device (Cook Medical Inc., Bjaeverskov, Denmark) were analyzed. Patients presenting with ruptured aortic complex aneurysms were characterized as emergent and patients with aneurysms >90 mm of diameter, or symptomatic aneurysms were characterized as urgent. Technical success, 30-day mortality, major adverse events (MAE) and spinal cord ischemia (SCI) rates were assessed.
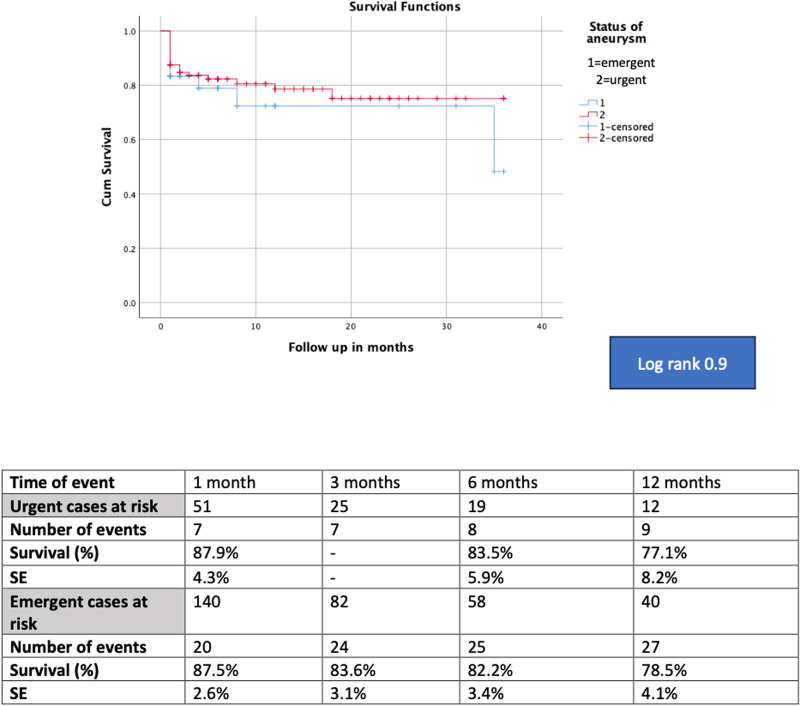
Results: 225 patients (36.5% females, 72.5 ± 2.8 years) were included; 73.0% were urgent. The mean aneurysm diameter was 109 ± 3.9 mm and 44.4% were type I-III TAAAs. Females (p = .03), para-renal aneurysms (p = .02) and ASA score IV (p < .001) were more common in emergent cases. Technical success was 97.8%. Thirty-day mortality and MAE rates were 17.8% and 30.6%, respectively. SCI rate was 14.7%, (4.8% paraplegia rate) with 22.2% of patients receiving prophylactic cerebrospinal drainage. Thirty-day mortality (13.3% vs. 26.7%, p = .04) and MAE (26.0% vs. 43.0%, p = .02) were more common among emergent cases while technical success (97.6% vs. 98.3%, p = .9), and SCI (13.3% vs. 18.3%, p = .4) were similar. Survival at 12-months was 83.5% (SE 5.9%) for the urgent and 77.1% (SE 8.2%) for the emergent group (log rank, p = 0.96).
Conclusion: T-Branch represents an effective and safe solution for the management of urgent and emergent cases with complex aortic aneurysms, with high technical success, promising early mortality and SCI rates.
Keywords: branched devices; complex endovascular repair; off-theshelf; ruptured; symptomatic; urgent.
© 2023 Nana, Spanos, Jakimowicz, Torrealba, Jama, Panuccio, Rohlffs and Kölbel.
Conflict of interest statement
TK is a consultant and proctor for and has intellectual property with Cook Medical, receiving royalties, speaking fees, and research, travel, and educational grants. TJ is a consultant and proctor for HammerMed—Polish distributor of Cook Medical, receiving royalties, speaking fees, and travel grants. All authors have completed the ICMJE uniform disclosure form and declare no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work; no other relationships or activities that could appear to have influenced the submitted work. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures

References
LinkOut - more resources
Full Text Sources