

Pretransplant BKV-IgG serostatus and BKV-specific ELISPOT assays to predict BKV infection after kidney transplantation
- PMID: 37809095
- PMCID: PMC10551174
- DOI: 10.3389/fimmu.2023.1243912
Pretransplant BKV-IgG serostatus and BKV-specific ELISPOT assays to predict BKV infection after kidney transplantation
Abstract
Introduction: Polyomavirus (BKV) infection can lead to major complications and damage to the graft in kidney transplant recipients (KTRs). We investigated whether pretransplant BK serostatus and BK-specific cell-mediated immunity (CMI) predicts post-transplant BK infection.
Methods: A total of 93 donor-recipient pairs who underwent kidney transplantation (KT) and 44 healthy controls were examined. Assessment of donor and recipient BKV serostatus and BKV-CMI in recipients was performed prior to transplantation using BKV-IgG ELISA and BKV-specific IFN-g ELISPOT assays against five BK viral antigens (LT, St, VP1, VP2, and VP3). BK viremia was diagnosed when blood BKV-DNA of 104 copies/mL or more was detected during follow-up periods.
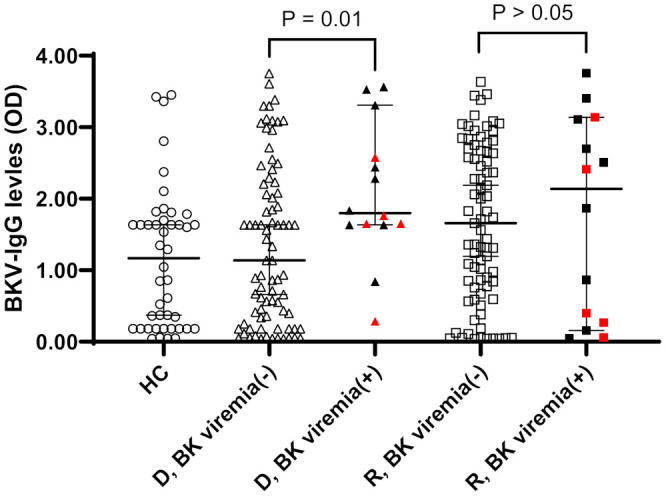
Results: Anti-BKV IgG antibody was detected in 74 (79.6%) of 93 KTRs and in 68 (73.1%) of 93 KT donors. A greater percentage of KTRs who received allograft from donors with high levels of anti-BKV IgG had posttransplant BK viremia (+) than KTRs from donors with low anti-BKV IgG (25.5% [12/47] vs. 4.3% [2/46], respectively; P = 0.007). Pretransplant total BKV-ELISPOT results were lower in BK viremia (+) patients than in patients without viremia (-) 20.5 [range 9.9-63.6] vs. 72.0 [43.2 - 110.8]; P = 0. 027). The sensitivity and specificity of the total BKV-ELISPOT assay (cut-off ≤ 53 spots/3×105 cells) for prediction of posttransplant BK viremia were 71.4 (95% CI: 41.9-91.6) and 54.4 (42.8-65.7), respectively. The combination of high donor BKV-IgG, low recipient BKV-IgG, and low total BKV-ELISPOT results improved specificity to 91.1%.
Discussion: Our study highlights the importance of pretransplant BKV-IgG serostatus and BKV-specific CMI in predicting posttransplant BKV infection in KTRs. The combination of high donor BKV-IgG, low recipient BKV-IgG, and low total BKV-ELISPOT results predicted BK viremia after KT. Pretransplant identification of patients at highrisk for BK viremia could enable timely interventions and improve clinical outcomes of KTRs.
Keywords: BK polyomavirus; BK viremia; BKV-specific ELISPOT; kidney transplant recipients; pre-transplant BKV-IgG serostatus.
Copyright © 2023 Bae, Jung, Chung, Yang and Oh.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Wunderink HF, van der Meijden E, van der Blij-de Brouwer CS, Mallat MJ, Haasnoot GW, van Zwet EW, et al. Pretransplantation donor-recipient pair seroreactivity against BK polyomavirus predicts viremia and nephropathy after kidney transplantation. Am J Transplant (2017) 17:161–72. doi: 10.1111/ajt.13880 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical