

Genetic testing for familial hyperparathyroidism: clinical-genetic profile in a Mediterranean cohort
- PMID: 37810884
- PMCID: PMC10558207
- DOI: 10.3389/fendo.2023.1244361
Genetic testing for familial hyperparathyroidism: clinical-genetic profile in a Mediterranean cohort
Abstract
Background: Approximately 10% of primary hyperparathyroidism cases are hereditary, due to germline mutations in certain genes. Although clinically relevant, a systematized genetic diagnosis is missing due to a lack of firm evidence regarding individuals to test and which genes to evaluate.
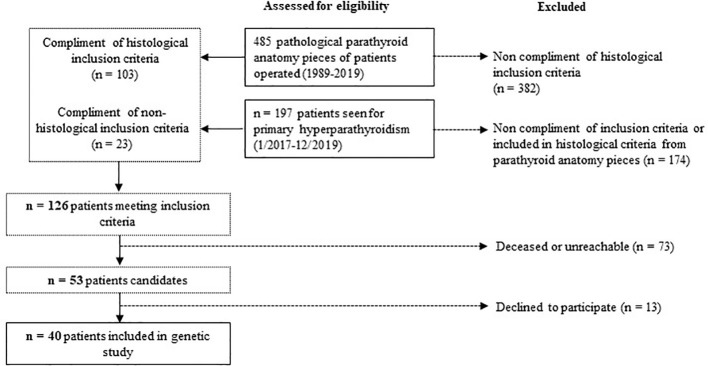
Methods: A customized gene panel (AIP, AP2S1, CASR, CDC73, CDKN1A, CDKN1B, CDKN2B, CDKN2C, GCM2, GNA11, MEN1, PTH, RET, and TRPV6) was performed in 40 patients from the Mediterranean area with suspected familial hyperparathyroidism (≤45 years of age, family history, high-risk histology, associated tumour, multiglandular disease, or recurrent hyperparathyroidism). We aimed to determine the prevalence of germline variants in these patients, to clinically characterize the probands and their relatives, and to compare disease severity in carriers versus those with a negative genetic test.
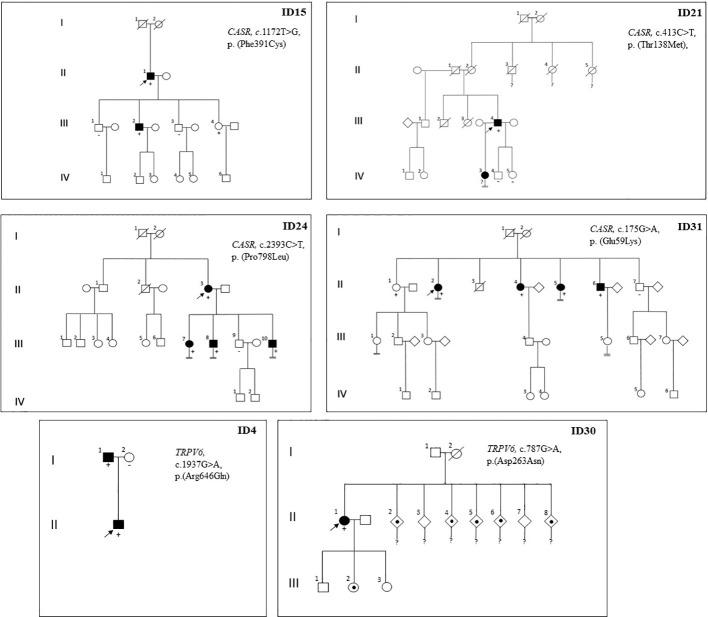
Results: Germline variants were observed in 9/40 patients (22.5%): 2 previously unknown pathogenic/likely pathogenic variants of CDKN1B (related to MEN4), 1 novel variant of uncertain significance of CDKN2C, 4 variants of CASR (3 pathogenic/likely pathogenic variants and 1 variant of uncertain significance), and 2 novel variants of uncertain significance of TRPV6. Familial segregation studies allowed diagnosis and early treatment of PHPT in first-degree relatives of probands.
Conclusion: The observed prevalence of germline variants in the Mediterranean cohort under study was remarkable and slightly higher than that seen in other populations. Genetic screening for suspected familial hyperparathyroidism allows the early diagnosis and treatment of PHPT and other related comorbidities. We recommend genetic testing for patients with primary hyperparathyroidism who present with high-risk features.
Keywords: cyclin-dependent kinase inhibitors; familial hyperparathyroidism; familial hypocalciuric hypercalcemia; multiple endocrine neoplasia type 1; multiple endocrine neoplasia type 4; parathyroid; primary hyperparathyroidism.
Copyright © 2023 Mazarico-Altisent, Capel, Baena, Bella-Cueto, Barcons, Guirao, Pareja, Muntean, Arsentales, Caixàs and Rigla.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Bilezikian JP, Brandi ML, Eastell R, Silverberg SJ, Udelsman R, Marcocci C, et al. Guidelines for the management of asymptomatic primary hyperparathyroidism: Summary statement from the fourth international workshop. J Clin Endocrinol Metab (2014) 99(10)3561–9. doi: 10.1210/jc.2014-1413 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous