

The Combination of Aroxybutynin and Atomoxetine in the Treatment of Obstructive Sleep Apnea (MARIPOSA): A Randomized Controlled Trial
- PMID: 37812772
- PMCID: PMC10765395
- DOI: 10.1164/rccm.202306-1036OC
The Combination of Aroxybutynin and Atomoxetine in the Treatment of Obstructive Sleep Apnea (MARIPOSA): A Randomized Controlled Trial
Erratum in
-
Erratum: Impact of Early Hemodynamic Screening on Extremely Preterm Outcomes in a High-Performance Center.Am J Respir Crit Care Med. 2024 Mar 15;209(6):767. doi: 10.1164/rccm.v209erratum4. Am J Respir Crit Care Med. 2024. PMID: 38488614 Free PMC article. No abstract available.
-
Erratum: The Combination of Aroxybutynin and Atomoxetine in the Treatment of Obstructive Sleep Apnea (MARIPOSA): A Randomized Controlled Trial.Am J Respir Crit Care Med. 2024 Mar 15;209(6):767. doi: 10.1164/rccm.v209erratum3. Am J Respir Crit Care Med. 2024. PMID: 38488615 Free PMC article. No abstract available.
Abstract
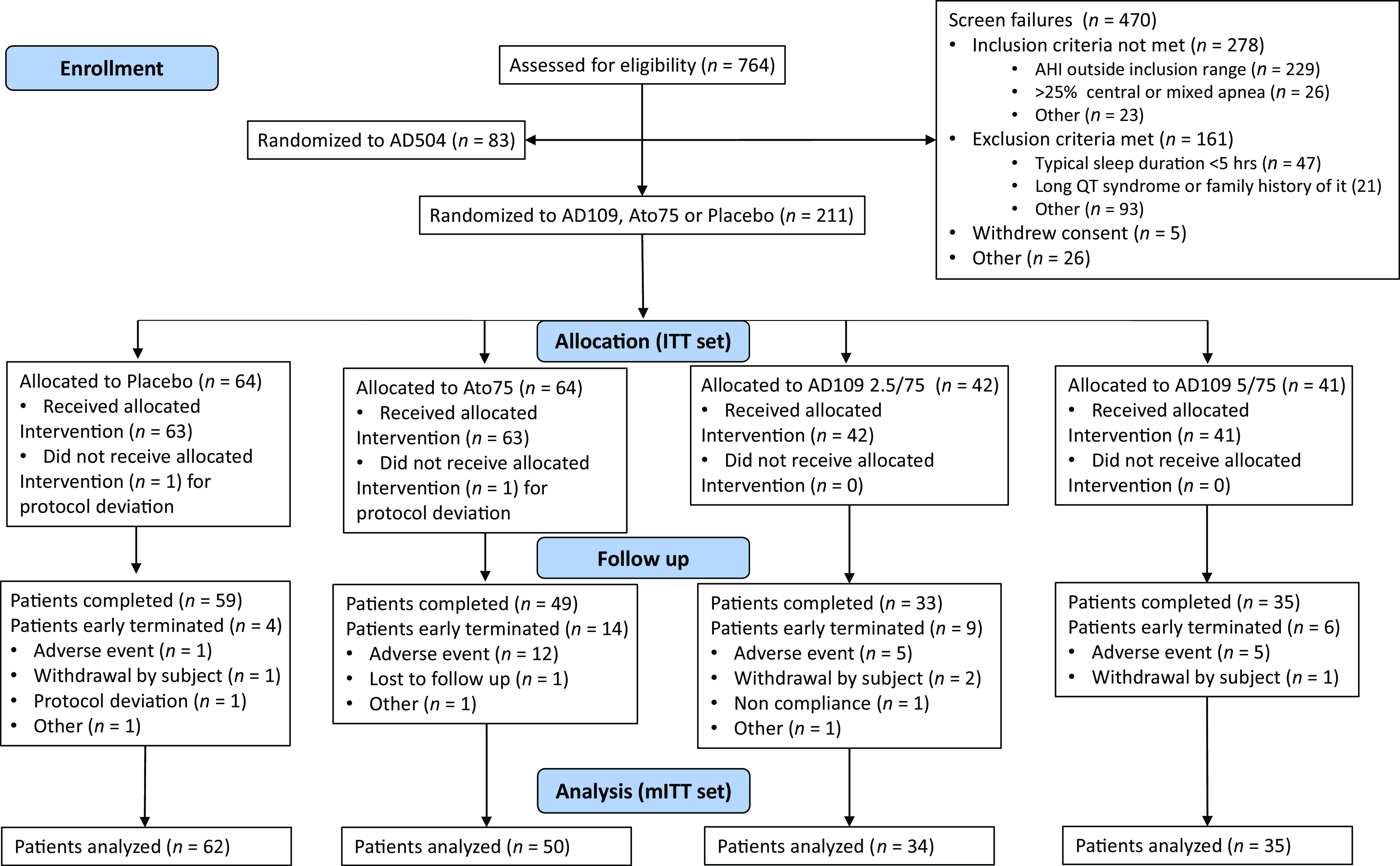
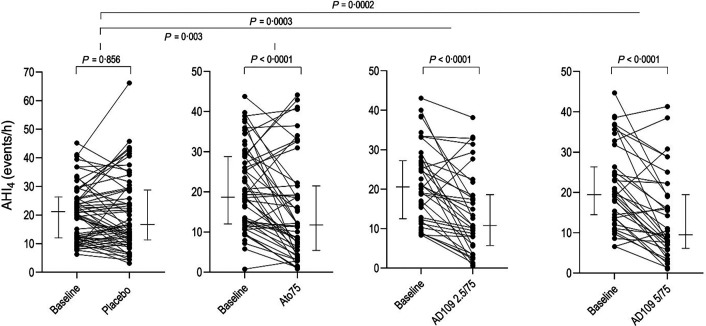
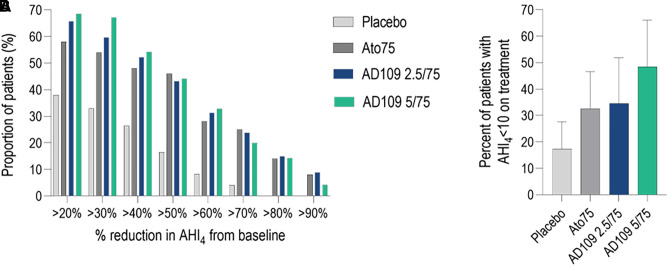
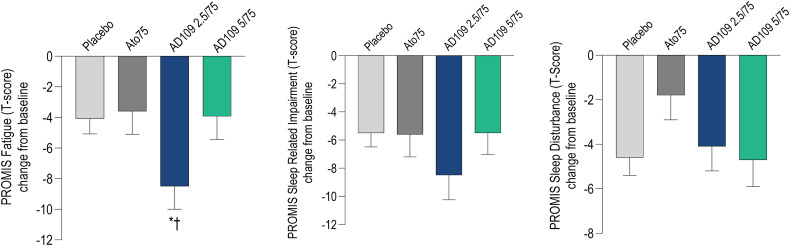
Rationale: Obstructive sleep apnea (OSA) is a common sleep disorder for which the principal treatment option, continuous positive airway pressure, is often poorly tolerated. There is currently no approved pharmacotherapy for OSA. However, recent studies have demonstrated improvement in OSA with combined antimuscarinic and noradrenergic drugs. Objectives: The aim of this study was to evaluate the efficacy and safety of AD109, a combination of the novel antimuscarinic agent aroxybutynin and the norepinephrine reuptake inhibitor atomoxetine, in the treatment of OSA. Methods: Phase II randomized, double-blind, placebo-controlled, parallel-group, 4-week trial comparing AD109 2.5/75 mg, AD109 5/75 mg, atomoxetine 75 mg alone, and placebo (www.clinicaltrials.gov identifier NCT05071612). Measurements and Main Results: Of 211 randomized patients, 181 were included in the prespecified efficacy analyses. Sleep was assessed by two baseline and two treatment polysomnograms. Apnea-hypopnea index with a 4% desaturation criterion (primary outcome) was reduced from a median (IQR) of 20.5 (12.3-27.2) to 10.8 (5.6-18.5) in the AD109 2.5/75 mg arm (-47.1%), from 19.4 (13.7-26.4) to 9.5 (6.1-19.3) in the AD109 5/75 mg arm (-42.9%; both P < 0.0001 vs. placebo), and from 19.0 (11.8-28.8) to 11.8 (5.5-21.5) with atomoxetine alone (-38.8%; P < 0.01 vs. placebo). Apnea-hypopnea index with a 4% desaturation criterion decreased from 20.1 (11.9-25.9) to 16.3 (11.1-28.9) in the placebo arm. Subjectively, there was improvement in fatigue with AD109 2.5/75 mg (P < 0.05 vs. placebo and atomoxetine). Atomoxetine taken alone decreased total sleep time (P < 0.05 vs. AD109 and placebo). The most common adverse events were dry mouth, insomnia, and urinary hesitancy. Conclusions: AD109 showed clinically meaningful improvement in OSA, suggesting that further development of the compound is warranted. Clinical trial registered with www.clinicaltrials.gov (NCT05071612).
Keywords: drug therapy; obstructive sleep apnea; pharmacology.
Figures
Comment in
-
Combination of Aroxybutynin and Atomoxetine in Obstructive Sleep Apnea: Is the Effect of One Plus One Greater than Two?Am J Respir Crit Care Med. 2024 Mar 15;209(6):763-764. doi: 10.1164/rccm.202310-1799LE. Am J Respir Crit Care Med. 2024. PMID: 38190697 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
