

Improvement of composite kidney outcomes by AKI care bundles: a systematic review and meta-analysis
- PMID: 37814334
- PMCID: PMC10563300
- DOI: 10.1186/s13054-023-04641-0
Improvement of composite kidney outcomes by AKI care bundles: a systematic review and meta-analysis
Abstract
Introduction: Various approaches have been suggested to identify acute kidney injury (AKI) early and to initiate kidney-protective measures in patients at risk or with AKI. The objective of this study was to evaluate whether care bundles improve kidney outcomes in these patients.
Methods: We conducted a systematic review of the literature to evaluate the clinical effectiveness of AKI care bundles with or without urinary biomarkers in the recognition and management of AKI. The main outcomes were major adverse kidney events (MAKEs) consisting of moderate-severe AKI, receipt of renal replacement therapy (RRT), and mortality.
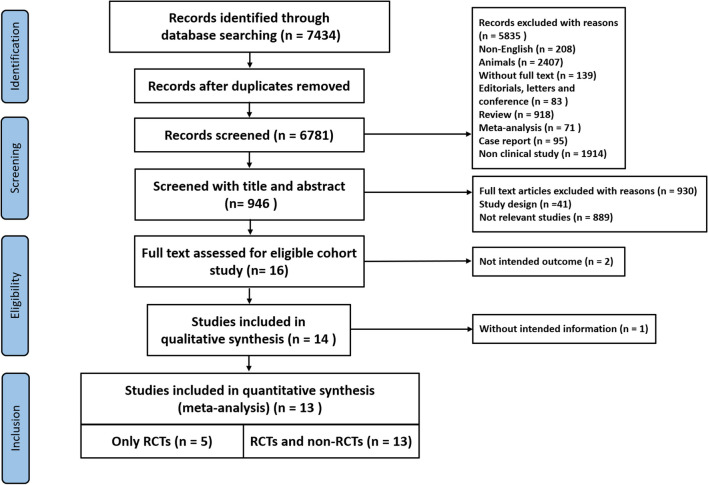
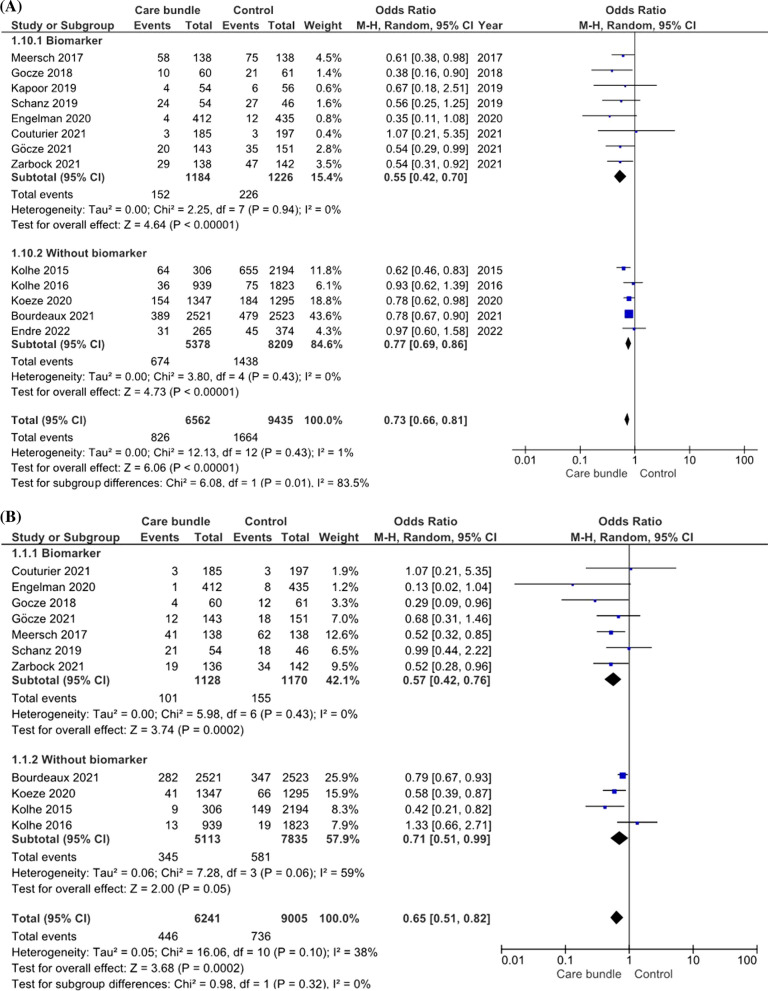
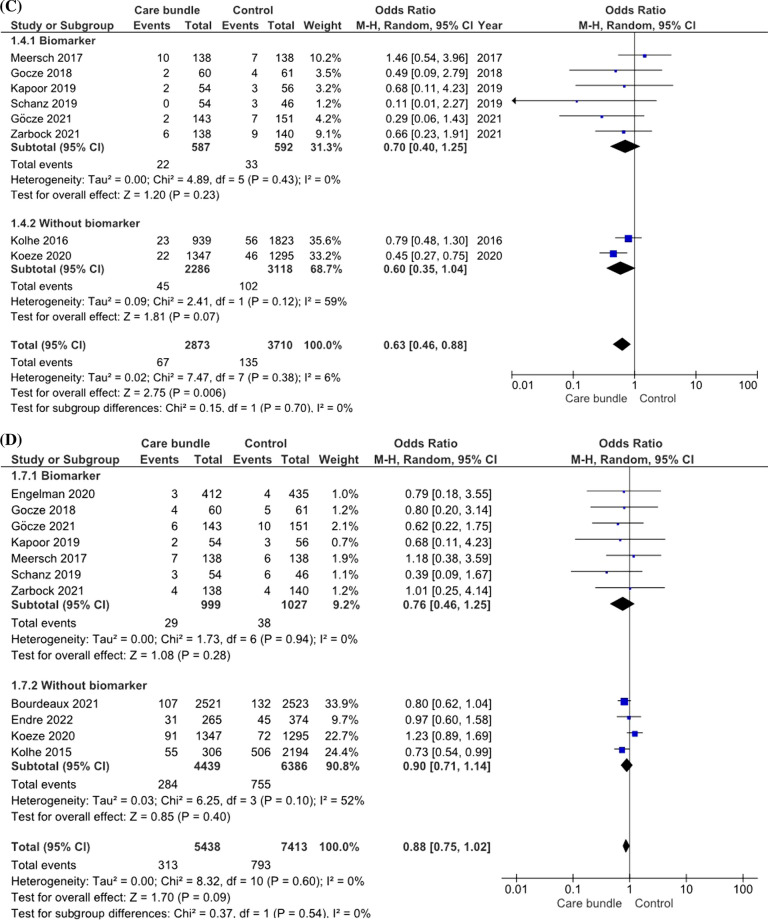
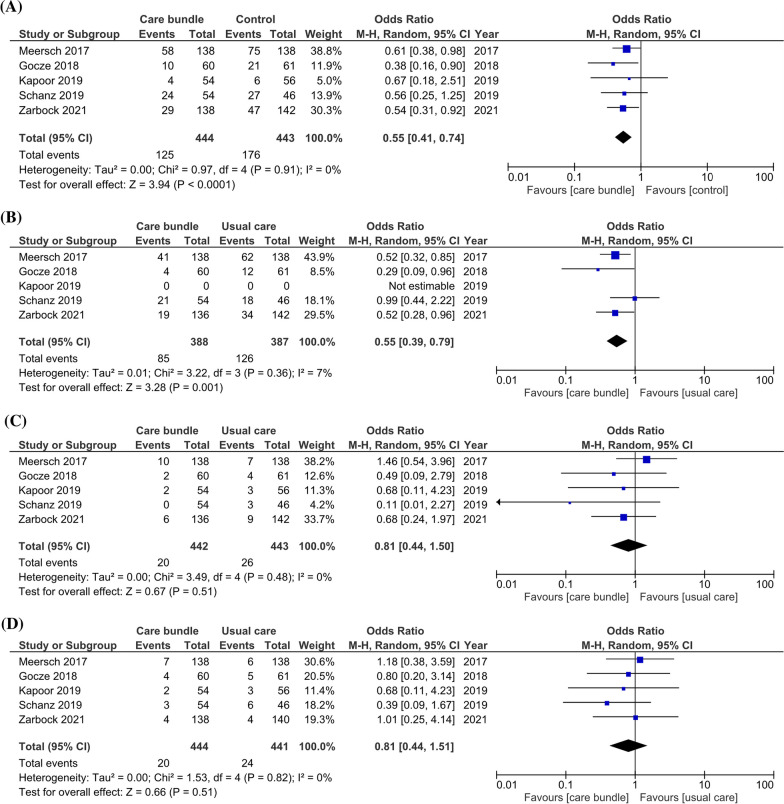
Results: Out of 7434 abstracts screened, 946 published studies were identified. Thirteen studies [five randomized controlled trials (RCTs) and eight non-RCTs] including 16,540 patients were eligible for inclusion in the meta-analysis. Meta-analysis showed a lower incidence of MAKE in the AKI care bundle group [odds ratio (OR) 0.73, 95% confidence interval (CI) 0.66-0.81] with differences in all 3 individual outcomes [moderate-severe AKI (OR 0.65, 95% CI 0.51-0.82), RRT (OR 0.63, 95% CI = 0.46-0.88) and mortality]. Subgroup analysis of the RCTs, all adopted biomarker-based approach, decreased the risk of MAKE (OR 0.55, 95% CI 0.41-0.74). Network meta-analysis could reveal that the incorporation of biomarkers in care bundles carried a significantly lower risk of MAKE when compared to care bundles without biomarkers (OR = 0.693, 95% CI = 0.50-0.96), while the usual care subgroup had a significantly higher risk (OR = 1.29, 95% CI = 1.09-1.52).
Conclusion: Our meta-analysis demonstrated that care bundles decreased the risk of MAKE, moderate-severe AKI and need for RRT in AKI patients. Moreover, the inclusion of biomarkers in care bundles had a greater impact than care bundles without biomarkers.
Keywords: Acute kidney injury; Biomarkers; Care bundles.
© 2023. BioMed Central Ltd., part of Springer Nature.
Conflict of interest statement
All authors declare no competing interest.
Figures
References
-
- Zarbock A, Nadim MK, Pickkers P, Gomez HA-O, Bell S, Joannidis MA-O, et al. Sepsis-associated acute kidney injury: consensus report of the 28th Acute Disease Quality Initiative workgroup. (1759–507X (Electronic)). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
