Modern Achalasia: Diagnosis, Classification, and Treatment
- PMID: 37814432
- PMCID: PMC10577462
- DOI: 10.5056/jnm23125
Modern Achalasia: Diagnosis, Classification, and Treatment
Abstract
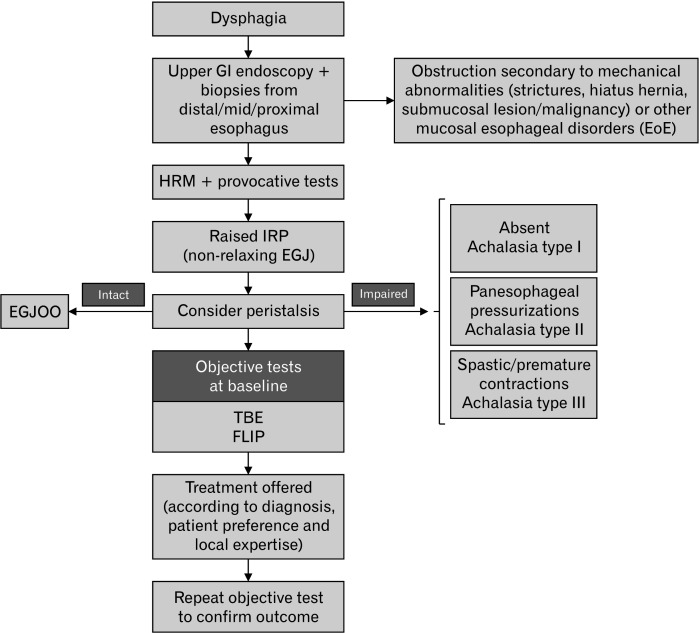
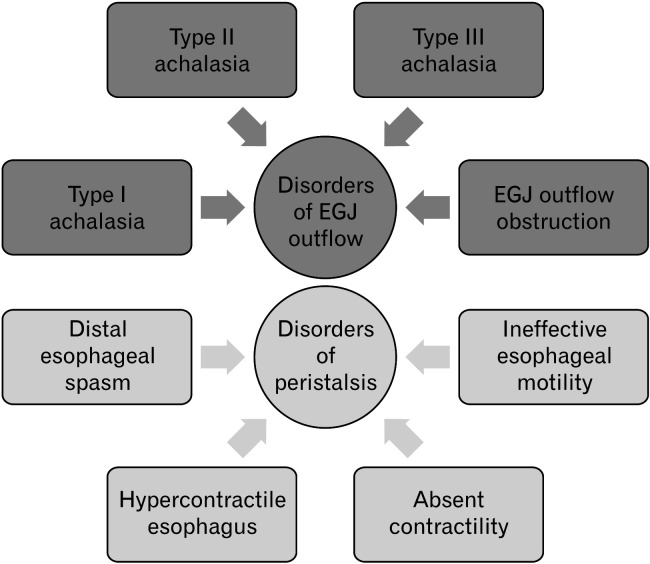
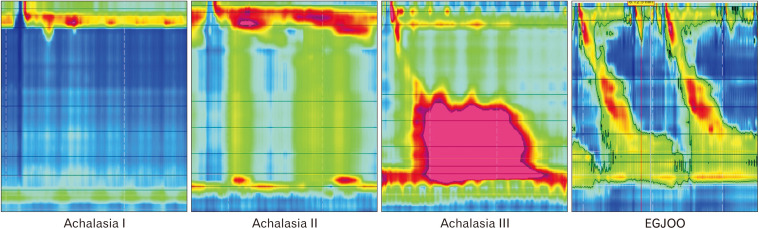
Achalasia is a major esophageal motor disorder featured by the altered relaxation of the esophagogastric junction in the absence of effective peristaltic activity. As a consequence of the esophageal outflow obstruction, achalasia patients present with clinical symptoms of dysphagia, chest pain, weight loss, and regurgitation of indigested food. Other less specific symptoms can also present including heartburn, chronic cough, and aspiration pneumonia. The delay in diagnosis, particularly when the presenting symptoms mimic those of gastroesophageal reflux disease, may be as long as several years. The widespread use of high-resolution manometry has permitted earlier detection and uncovered achalasia phenotypes which can have prognostic and therapeutic implications. Other tools have also emerged to help define achalasia severity and which can be used as objective measures of response to therapy including the timed barium esophagogram and the functional lumen imaging probe. Such diagnostic innovations, along with the increased awareness by clinicians and patients due to the availability of alternative therapeutic approaches (laparoscopic and robotic Heller myotomy, and peroral endoscopic myotomy) have radically changed the natural history of the disorder. Herein, we report the most recent advances in the diagnosis, classification, and management of esophageal achalasia and underline the still-grey areas that needs to be addressed by future research to reach the goal of personalizing treatment.
Keywords: Barium; Esophageal achalasia; Heller myotomy.
Conflict of interest statement
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials