

Diagnostic Criteria for Identifying Individuals at High Risk of Progression From Mild or Moderate to Severe Alcohol Use Disorder
- PMID: 37815828
- PMCID: PMC10565602
- DOI: 10.1001/jamanetworkopen.2023.37192
Diagnostic Criteria for Identifying Individuals at High Risk of Progression From Mild or Moderate to Severe Alcohol Use Disorder
Abstract
Importance: Current Diagnostic and Statistical Manual of Mental Disorders (Fifth Edition) (DSM-5) diagnoses of substance use disorders rely on criterion count-based approaches, disregarding severity grading indexed by individual criteria.
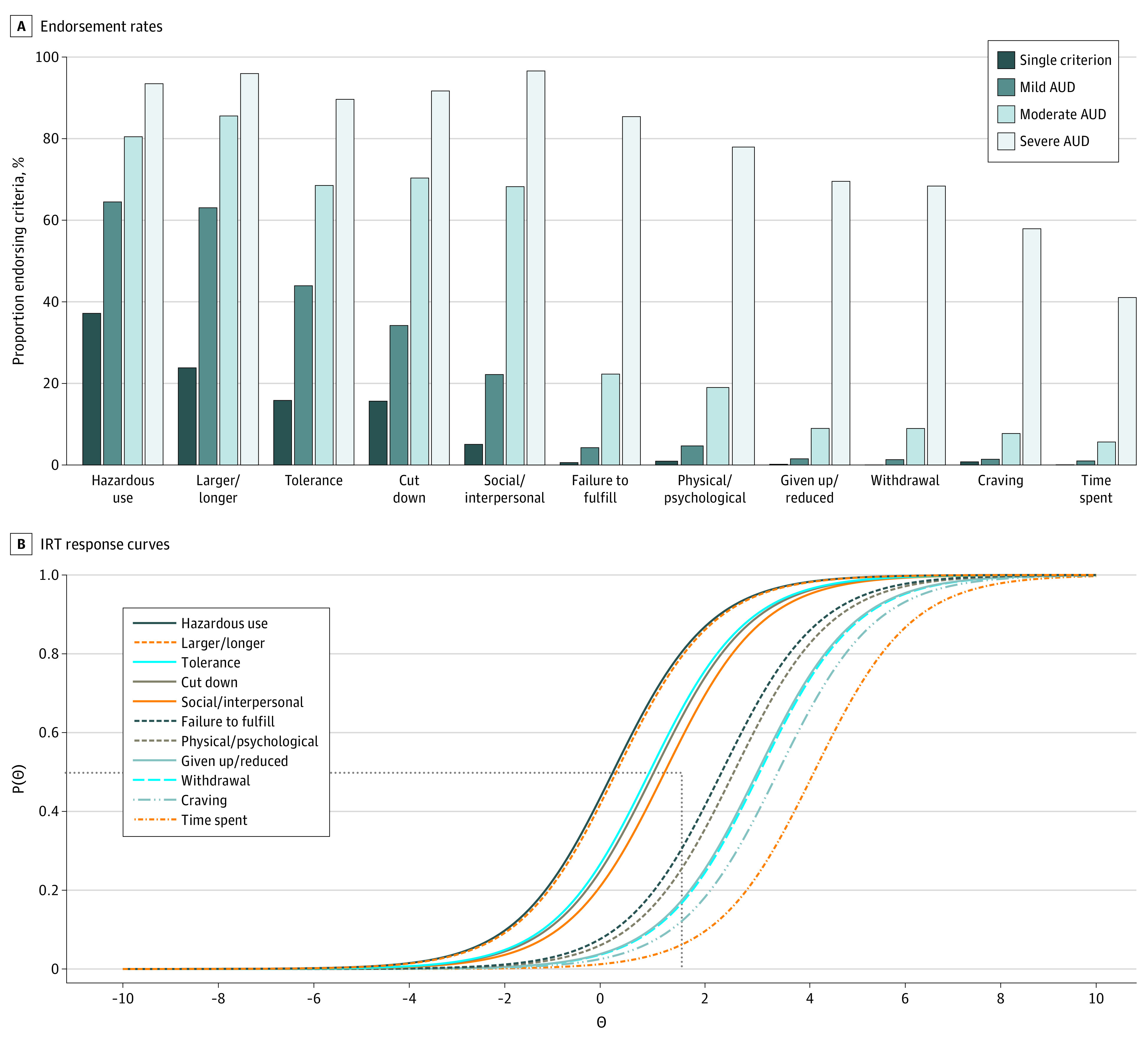
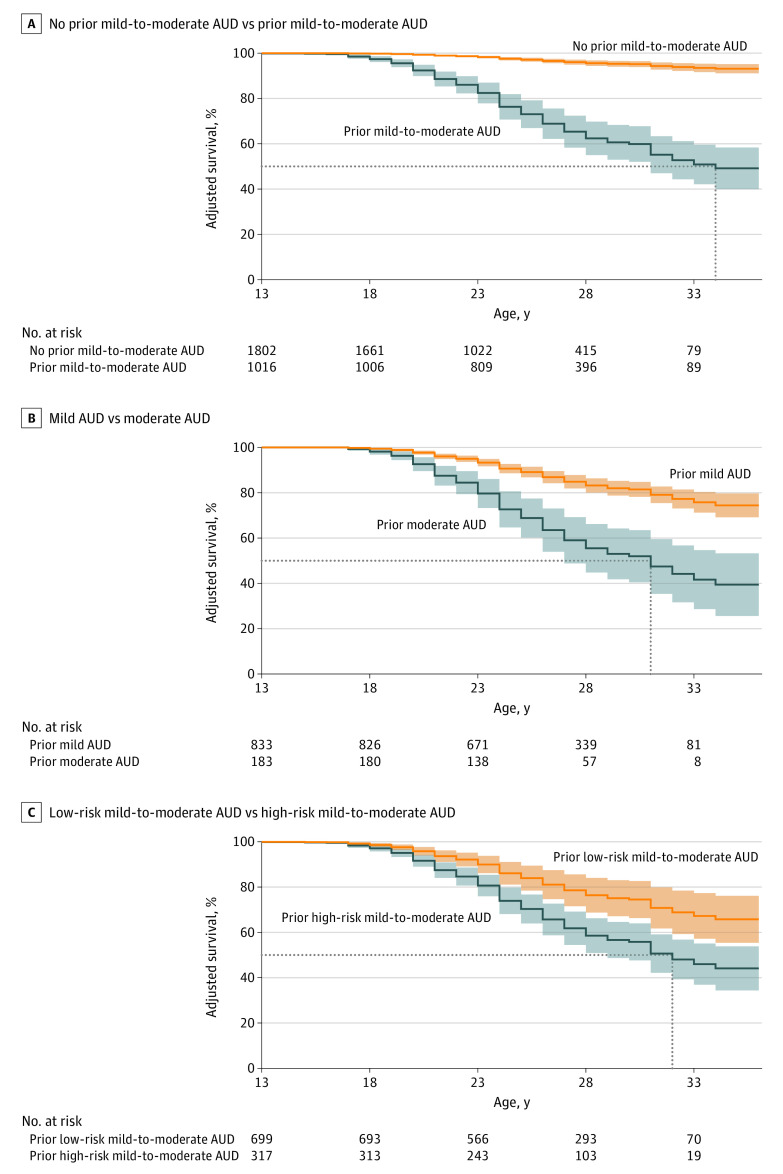
Objective: To examine correlates of alcohol use disorder (AUD) across count-based severity groups (ie, mild, moderate, mild-to-moderate, severe), identify specific diagnostic criteria indicative of greater severity, and evaluate whether specific criteria within mild-to-moderate AUD differentiate across relevant correlates and manifest in greater hazards of severe AUD development.
Design, setting, and participants: This cohort study involved 2 cohorts from the family-based Collaborative Study on the Genetics of Alcoholism (COGA) with 7 sites across the United States: cross-sectional (assessed 1991-2005) and longitudinal (assessed 2004-2019). Statistical analyses were conducted from December 2022 to June 2023.
Main outcomes and measures: Sociodemographic, alcohol-related, psychiatric comorbidity, brain electroencephalography (EEG), and AUD polygenic score measures as correlates of DSM-5 AUD levels (ie, mild, moderate, severe) and criterion severity-defined mild-to-moderate AUD diagnostic groups (ie, low-risk vs high-risk mild-to-moderate).
Results: A total of 13 110 individuals from the cross-sectional COGA cohort (mean [SD] age, 37.8 [14.2] years) and 2818 individuals from the longitudinal COGA cohort (mean baseline [SD] age, 16.1 [3.2] years) were included. Associations with alcohol-related, psychiatric, EEG, and AUD polygenic score measures reinforced the role of increasing criterion counts as indexing severity. Yet within mild-to-moderate AUD (2-5 criteria), the presence of specific high-risk criteria (eg, withdrawal) identified a group reporting heavier drinking and greater psychiatric comorbidity even after accounting for criterion count differences. In longitudinal analyses, prior mild-to-moderate AUD characterized by endorsement of at least 1 high-risk criterion was associated with more accelerated progression to severe AUD (adjusted hazard ratio [aHR], 11.62; 95% CI, 7.54-17.92) compared with prior mild-to-moderate AUD without endorsement of high-risk criteria (aHR, 5.64; 95% CI, 3.28-9.70), independent of criterion count.
Conclusions and relevance: In this cohort study of a combined 15 928 individuals, findings suggested that simple count-based AUD diagnostic approaches to estimating severe AUD vulnerability, which ignore heterogeneity among criteria, may be improved by emphasizing specific high-risk criteria. Such emphasis may allow better focus on individuals at the greatest risk and improve understanding of the development of AUD.
Conflict of interest statement
Figures
References
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
-
- Substance Abuse and Mental Health Services Administration . Key substance use and mental health indicators in the United States: results from the 2021 National Survey on Drug Use and Health [HHS Publ No PEP22-07-005, NSDUH Ser H-57]. Accessed September 7, 2023. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
