

Heterogeneous cardiac sympathetic innervation gradients promote arrhythmogenesis in murine dilated cardiomyopathy
- PMID: 37815863
- PMCID: PMC10721311
- DOI: 10.1172/jci.insight.157956
Heterogeneous cardiac sympathetic innervation gradients promote arrhythmogenesis in murine dilated cardiomyopathy
Abstract
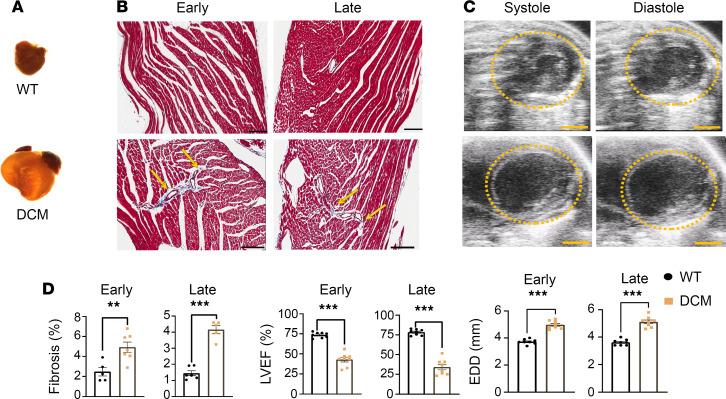
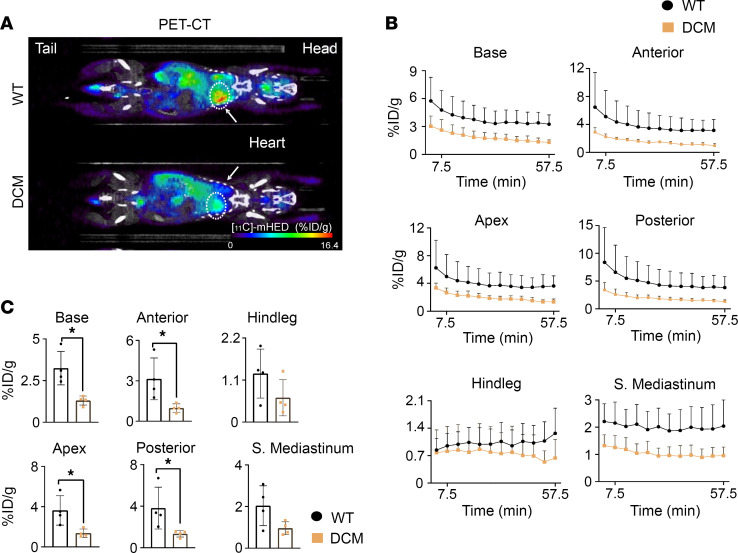
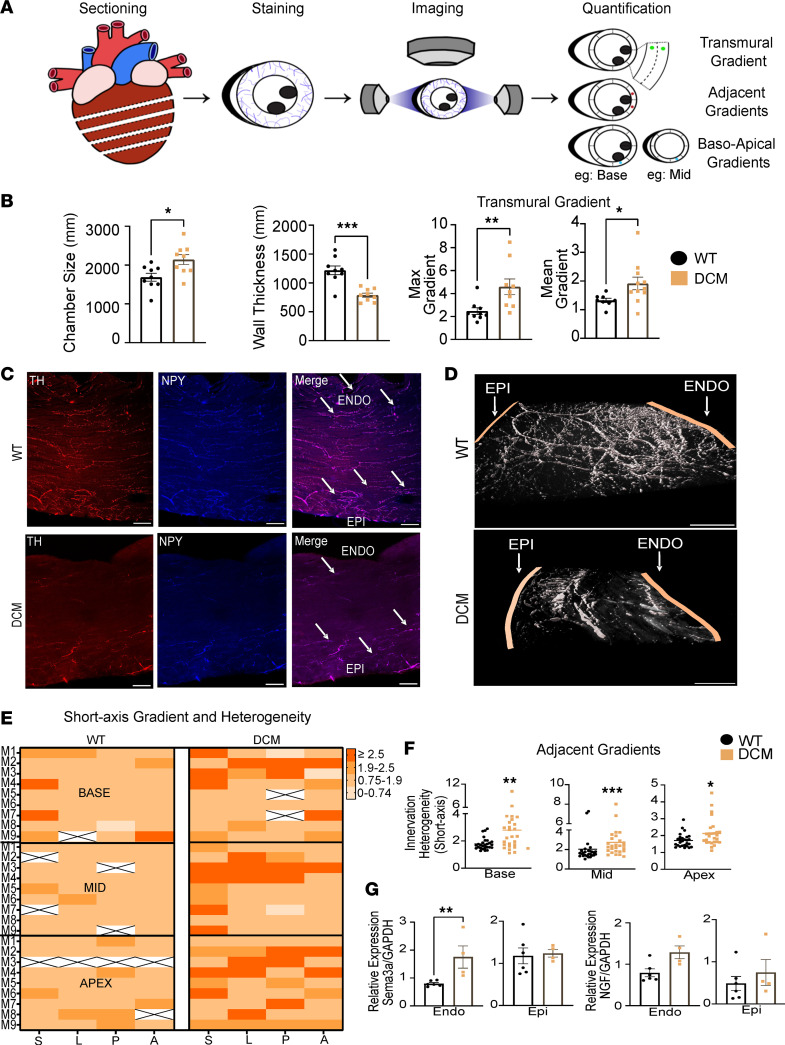
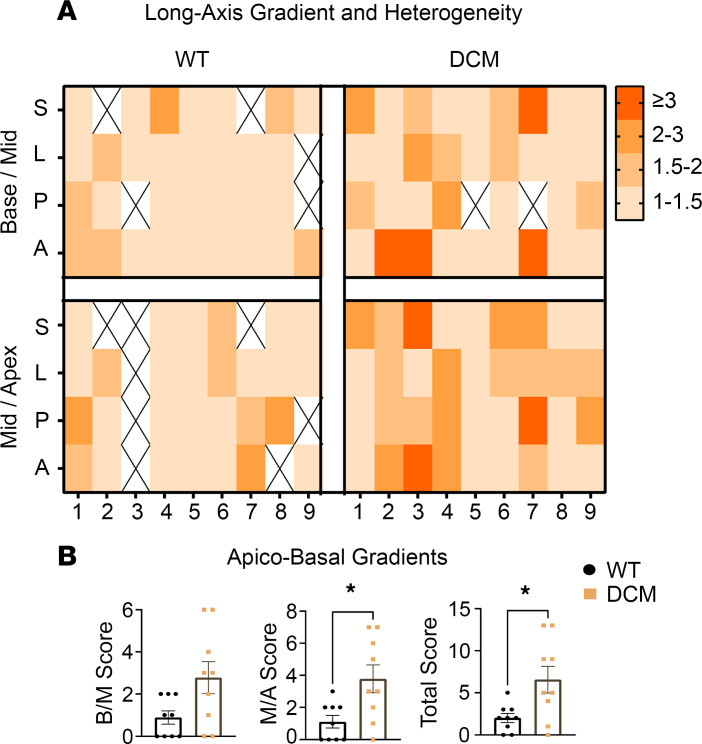
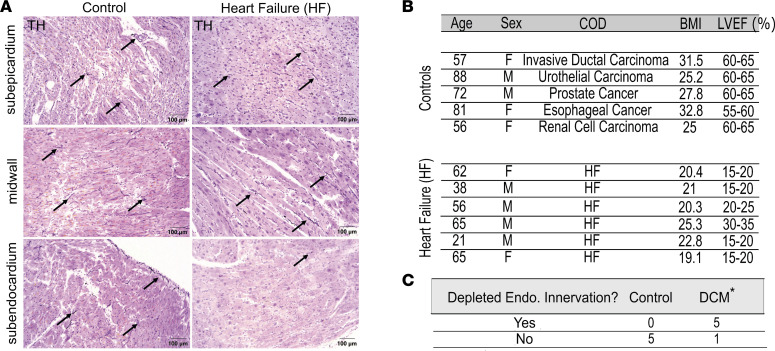
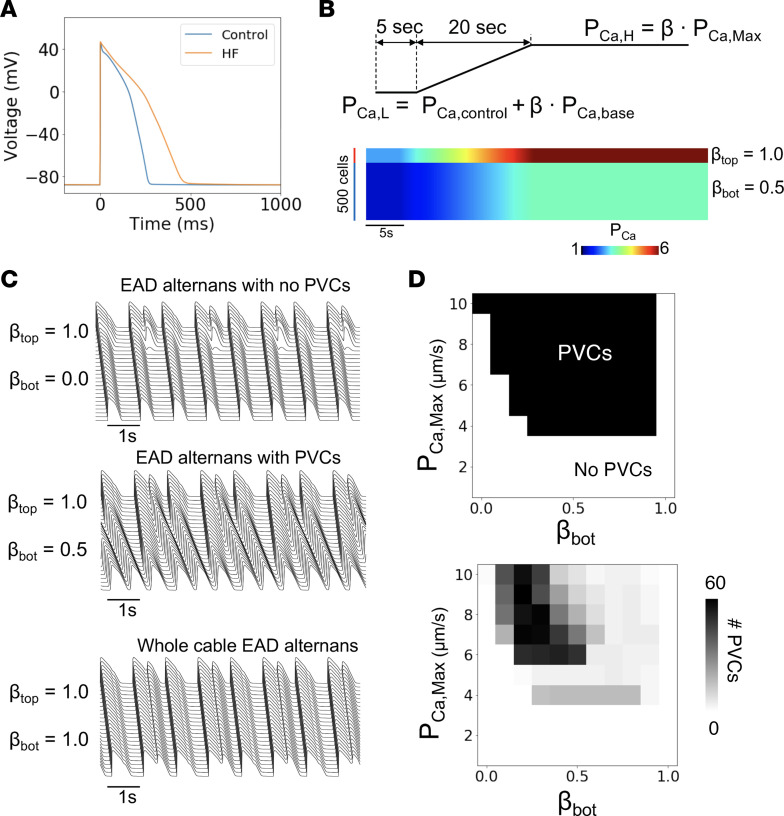
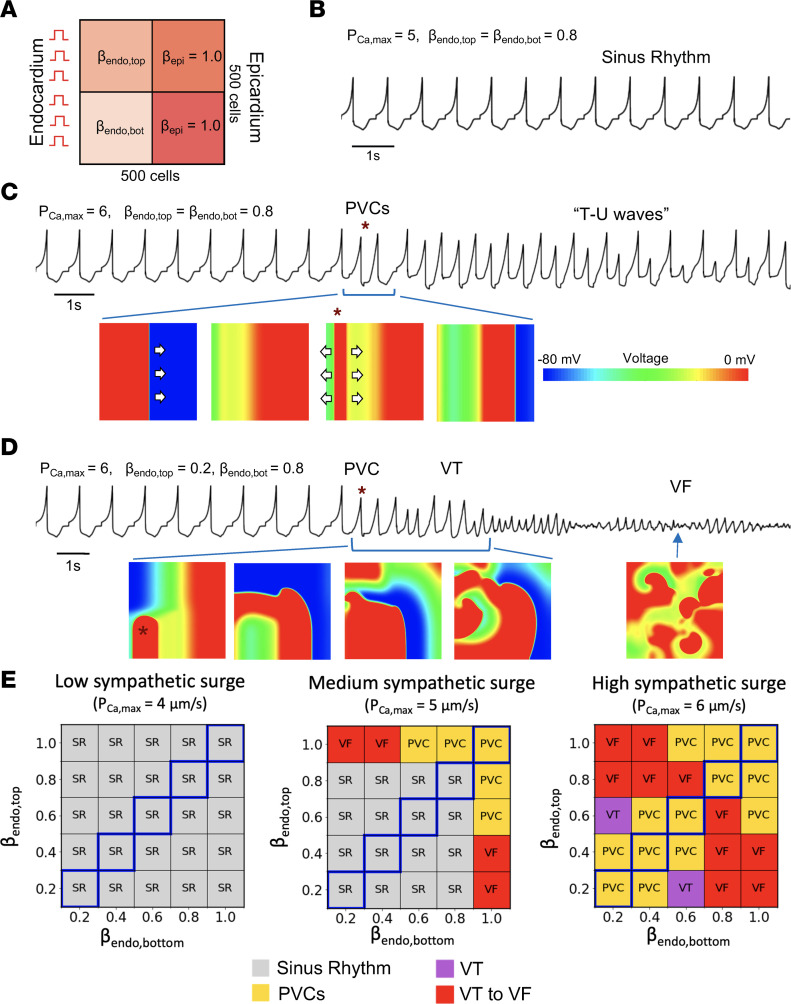
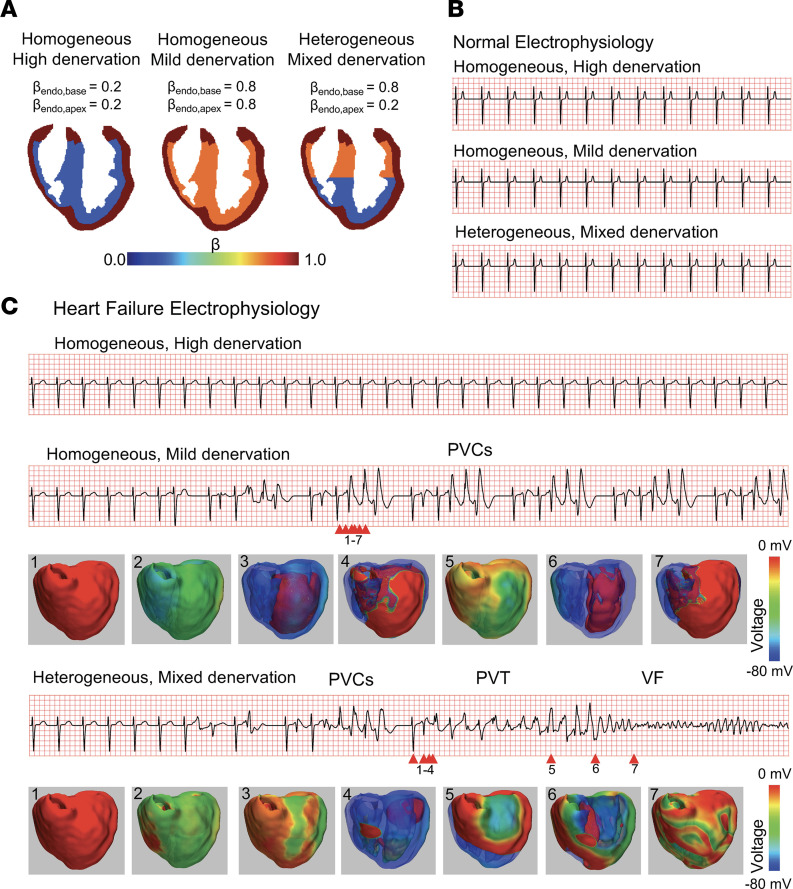
Ventricular arrhythmias (VAs) in heart failure are enhanced by sympathoexcitation. However, radiotracer studies of catecholamine uptake in failing human hearts demonstrate a proclivity for VAs in patients with reduced cardiac sympathetic innervation. We hypothesized that this counterintuitive finding is explained by heterogeneous loss of sympathetic nerves in the failing heart. In a murine model of dilated cardiomyopathy (DCM), delayed PET imaging of sympathetic nerve density using the catecholamine analog [11C]meta-Hydroxyephedrine demonstrated global hypoinnervation in ventricular myocardium. Although reduced, sympathetic innervation in 2 distinct DCM models invariably exhibited transmural (epicardial to endocardial) gradients, with the endocardium being devoid of sympathetic nerve fibers versus controls. Further, the severity of transmural innervation gradients was correlated with VAs. Transmural innervation gradients were also identified in human left ventricular free wall samples from DCM versus controls. We investigated mechanisms underlying this relationship by in silico studies in 1D, 2D, and 3D models of failing and normal human hearts, finding that arrhythmogenesis increased as heterogeneity in sympathetic innervation worsened. Specifically, both DCM-induced myocyte electrical remodeling and spatially inhomogeneous innervation gradients synergistically worsened arrhythmogenesis. Thus, heterogeneous innervation gradients in DCM promoted arrhythmogenesis. Restoration of homogeneous sympathetic innervation in the failing heart may reduce VAs.
Keywords: Arrhythmias; Cardiology; Heart failure; Neurodegeneration.
Conflict of interest statement
Figures

References
-
- Ieda M, Fukuda K. New aspects for the treatment of cardiac diseases based on the diversity of functional controls on cardiac muscles: the regulatory mechanisms of cardiac innervation and their critical roles in cardiac performance. J Pharmacol Sci. 2009;109(3):348–353. doi: 10.1254/jphs.08R25FM. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
