

Clinical practice guideline for management of osteoporosis and fracture prevention in Canada: 2023 update
- PMID: 37816527
- PMCID: PMC10610956
- DOI: 10.1503/cmaj.221647
Clinical practice guideline for management of osteoporosis and fracture prevention in Canada: 2023 update
Abstract
Background: In Canada, more than 2 million people live with osteoporosis, a disease that increases the risk for fractures, which result in excess mortality and morbidity, decreased quality of life and loss of autonomy. This guideline update is intended to assist Canadian health care professionals in the delivery of care to optimize skeletal health and prevent fractures in postmenopausal females and in males aged 50 years and older.
Methods: This guideline is an update of the 2010 Osteoporosis Canada clinical practice guideline on the diagnosis and management of osteoporosis in Canada. We followed the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework and quality assurance as per Appraisal of Guidelines for Research and Evaluation (AGREE II) quality and reporting standards. Primary care physicians and patient partners were represented at all levels of the guideline committees and groups, and participated throughout the entire process to ensure relevance to target users. The process for managing competing interests was developed before and continued throughout the guideline development, informed by the Guideline International Network principles. We considered benefits and harms, patient values and preferences, resources, equity, acceptability and feasibility when developing recommendations; the strength of each recommendation was assigned according to the GRADE framework.
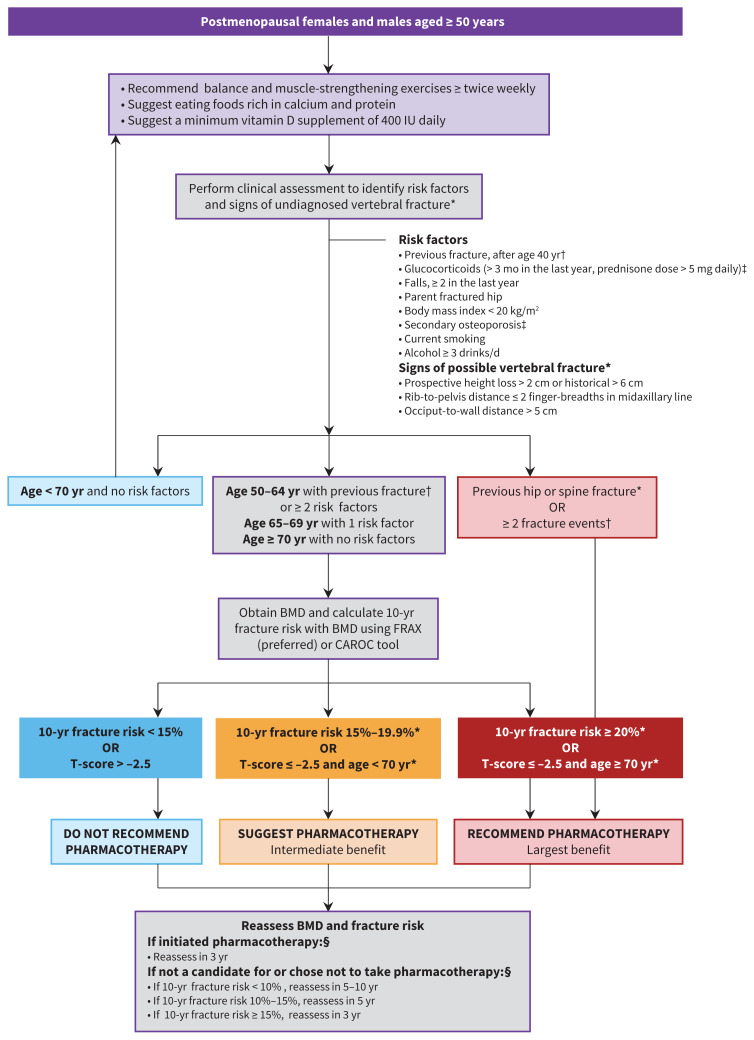
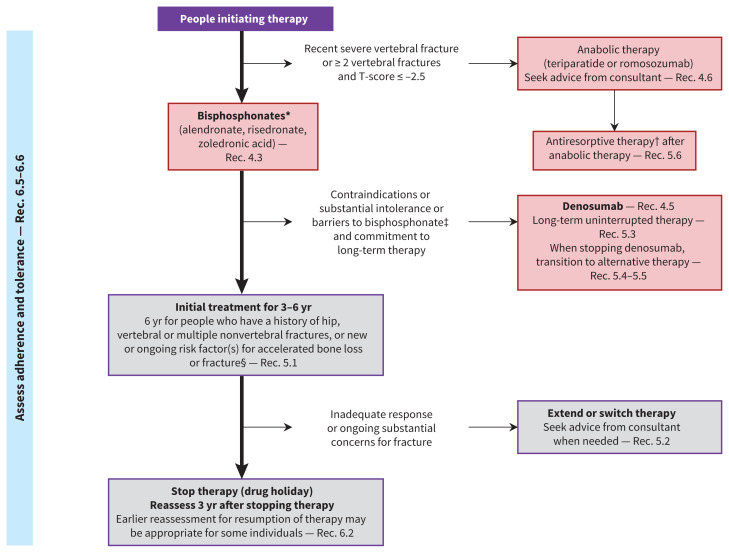
Recommendations: The 25 recommendations and 10 good practice statements are grouped under the sections of exercise, nutrition, fracture risk assessment and treatment initiation, pharmacologic interventions, duration and sequence of therapy, and monitoring. The management of osteoporosis should be guided by the patient's risk of fracture, based on clinical assessment and using a validated fracture risk assessment tool. Exercise, nutrition and pharmacotherapy are key elements of the management strategy for fracture prevention and should be individualized.
Interpretation: The aim of this guideline is to empower health care professionals and patients to have meaningful discussions on the importance of skeletal health and fracture risk throughout older adulthood. Identification and appropriate management of skeletal fragility can reduce fractures, and preserve mobility, autonomy and quality of life.
© 2023 CMA Impact Inc. or its licensors.
Conflict of interest statement
Competing interests: Lora Giangregorio reports receiving an honorarium from Amgen Inc. for a lecture on exercise with no mention of medications, outside the current manuscript. Dr. Giangregorio is also a member of the Scientific Advisory Council of Osteoporosis Canada and co-lead of the Vertebral Fracture Special Interest Group, Fragility Fracture Network. Sandra Kim reports receiving support from Osteoporosis Canada for a Grading of Recommendations, Assessment, Development and Evaluations (GRADE) methodologist at McMaster University, during the conduct of the study. Dr. Kim was also a volunteer member of the Osteoporosis Canada Board of Directors from 2017 to 2020. Nancy Santesso reports receiving payment to provide GRADE expertise for guideline development and preparation of materials paid to institution (McMaster University), during the conduct of the study. Dr. Santesso has also received support from Osteoporosis Canada for travel to guideline-related meetings. Heather McDonald-Blumer reports receiving consulting fees from Eli Lilly and Novartis, for attendance on advisory boards, outside the submitted work. Rowena Ridout has been a member of the Osteoporosis Canada Board of Directors since 2020 (no payment received). Neil Binkley reports receiving a research grant (paid to institution) from Radius, and consulting fees and honoraria from Amgen. Angela Cheung has received honoraria for consultancy work from Amgen and Paladin Laboratories. Dr. Cheung has also held the following roles: member of the Clinical Guidelines Committee of the Endocrine Society; co-chair of the postmenopausal health pathway, American College of Obstetrics and Gynecology; and vice-president and co-chair of the 2023 Position Development Conference, International Society for Clinical Densitometry. Robert Josse reports receiving consulting fees from Amgen Canada, Paladin Laboratories and Alexion, and honoraria from Amgen and Alexion. Dr. Josse has also participated on advisory boards for Amgen, Paladin, Alexion and Ultragenyx. Aliya Khan has received research grants from Alexion, Amgen Canada, Takeda, Ascendis, Chugai, Radius, Amolyt and Ultragenyx, and speaker honoraria from Amgen, Alexion, Ascendis, Takeda and Ultragenyx. Dr. Khan has also participated on advisory boards for Amgen Canada, Alexion, Amolyt, Ascendis and Takeda. E. Lynn Izumi Nash reports receivin an honorarium from the Ontario College of Family Physicians for designing continuing medical education workshops on osteoporosis. Dr. Nash is also a member of the Scientific Advisory Council for Osteoporosis Canada (voluntary unpaid position). Zahra Bardai reports receiving honoraria as a member of the Pri-Med Canada Scientific Planning Committee (2011–present) and as an author of the Foundation for Medical Practice Education Small Group Practice–Based Learning Program, at McMaster University. Dr. Bardai is also a volunteer member of the Osteoporosis Canada Scientific Advisory Council. Suzanne Cadarette reports receiving research funds (paid to institution) as co–principal investigator on Canadian Institutes of Health Research and National Institutes of Health project grants. Heather Frame is a former member of the Osteoporosis Canada Board of Directors (term ended November 2020). Kaleen Hayes reports receiving researcher-initiated grants from the National Institute on Aging, Insight Therapeutics, Genentech and Sanofi (all paid directly to institution), and consulting fees from the Canadian Agency for Drugs and Technologies in Health. Alexandra Papaioannou has participated on an advisory board and in speakers’ bureaus and received honoraria from Amgen Canada. Christine Thomas has been a member of the Osteoporosis Canada Board of Directors at various time points. Conflict-of-Interest Oversight Committee: Heather McDonald-Blumer (Chair), Larry Funnell, Rowena Ridout.
Figures
References
-
- Osteoporosis and related fractures in Canada: report from the Canadian Chronic Disease Surveillance System. Ottawa: Public Health Agency of Canada; 2020:1–85. Available: https://www.canada.ca/content/dam/phac-aspc/documents/services/publicati... (accessed 2023 May 15).
-
- Adler RA. Update on osteoporosis in men. Best Pract Res Clin Endocrinol Metab 2018;32:759–72. - PubMed
-
- Siminoski K, Leslie WD, Frame H, et al. Canadian Association of Radiologists. Recommendations for bone mineral density reporting in Canada. Can Assoc Radiol J 2005;56:178–88. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical