We confirm that we have read the Journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
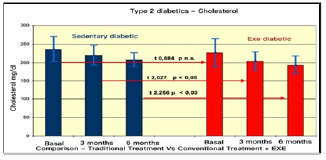
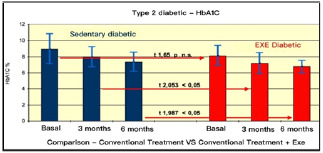
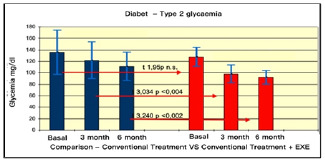
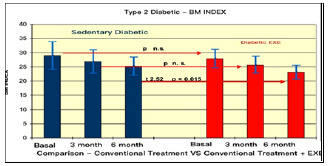
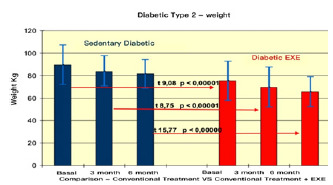
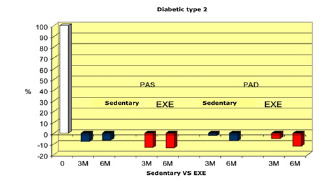
Diabetes mellitus (DM) is a chronic disease that includes a group of conditions characterised by increased blood glucose concentration. Depending on the age of onset, it is classified into type 1 diabetes mellitus (T1DM) and type 2 diabetes mellitus (T2DM). It is becoming an epidemic in some countries of the world, with the number of people affected expected to double in the next decade as the population ages. Is probably one of the oldest diseases known to man and it was first reported in Egyptian manuscript about 3000 years ago. T1DM is a chronic autoimmune disease characterised by a lack of or inadequate production and/or action of insulin, due to a dysfunction of the β cells of the endocrine pancreas and consequent hyperglycaemia. There are conflicting studies on the association between the onset of T1DM and a prolonged increase in body mass index (BMI) in the paediatric population, identified at the 85th percentile in growth curves. However, lifestyle modifications could delay the onset of the disease in these at-risk individuals. Although T1DM manifests itself as an acute event at a young age, the disease can reveal itself at any age and up to 50% of cases occur in adulthood. While, regarding T2DM was first described as a component of metabolic syndrome in 1988. It is estimated that by 2030, 552 million people will be affected by DM. In this metabolic alteration, age, gender, obesity, hypertension, genetics, diet, smoking, alcohol, sedentary lifestyle are risk factors. Several novel medications are in development, but the greatest need is for agents that enhance insulin sensitivity, halt the progressive pancreatic β-cell failure that is characteristic of T2DM and prevent or reverse the microvascular complications. Various lifestyle factors are known to be important to the development of the T2DM and of these obesity is neither an innocent bystander nor an occasional accomplice to diabetes, but it is a primary risk factor, in fact has been found to contribute to approximately 55% of cases of type 2 DM. Seventy percent of the western population is not active enough to maintain optimal health and weight. In the last twenty years obesity levels have tripled, (20% of men and 10-25% of women are obese). This tendency is caused by a decrease in physical activity (PA). In the last decade, the attention of the Italian diabetological community, has focused on the quality of life (QoL), PA and sports, thanks also to the promotional impulse given by the Italian Association of Diabetic Athletes. Various modalities of training can alter insulin action in a short period of time and an association of dietary programs, can improve the effects of the training to reverse the metabolism syndrome. In addition, numerous studies showed that the effects of obesity on glucose metabolism lead to impaired glucose tolerance, the development of insulin resistance and the consequent damage to the secretory function of β-cells. Keeping the weight fit is, therefore, a matter of intake and energy expenditure, because overweight and obesity develop when the energy intake is higher for a prolonged period. According to a World Health Organization (WHO) ranking, the prevalence of obesity in the United States increased from 30.5% to 41.9% during the period between from March 1999-2000 and during the same period between 2017-2020. The WHO defines a normal weight individual for an BMI 18.5 kg/m2 and < 25 kg/m2, underweight if < 18.5 kg/m2, overweight if 25 kg/m2 and obese if 30 kg/m2. The risk of the T2DM rises linearly with an increase in body mass index which, in concert, induces a constellation of metabolic abnormalities such as dyslipidaemia, cardiovascular morbidity and mortality. More than 95% of people with diabetes have T2DM, which is largely the result of excess body weight and physical inactivity. People with impaired glucose tolerance (IGT) or impaired fasting glycaemia (IFG) are at high risk of progressing to T2DM, although this is not inevitable. The worldwide increase in the prevalence of obesity is likely responsible for the recent increase in the prevalence of type 2 diabetes. A correct diagnosis is the fundamental prerequisite to identify the persons to be addressed to the diagnostic and therapeutic paths of care (PDTA). In T2DM there is a relative insulin deficiency caused by pancreatic β-cell dysfunction and insulin resistance in target organs. This leads to a decrease in glucose transport into the liver, muscle cells, and fat cells. As a result of this dysfunction, glucagon and hepatic glucose levels that rise during fasting are not suppressed with a meal. Given inadequate levels of insulin and increased insulin resistance, hyperglycemia results. A diagnosis of diabetes is based on a fasting blood glucose concentration above 7·0 mmol/L (126 mg/dL), a random blood glucose concentrate on above 11·1 mmol/L (200 mg/dl) with symptoms, or an abnormal result from an oral glucose tolerance test. The incretins are important gut mediators of insulin release, and in the case of the glucagon-like peptide 1 (GLP-1), of glucagon suppression. GLP-1 insulinotropic effects are preserved, and thus GLP-1 represents a potentially beneficial therapeutic option. Both classes of agents have shown not only to have the ability to normalize fasting and post-prandial glucose levels, but also to improve the functioning and mass of β cells. Furthermore, based on the established health benefits of PA and a healthy diet in a recent review Proia et al, highlighted the role of these gut peptides in bone and glucose metabolism. Indeed, they are able to respond to food intake and trigger regulatory mechanisms in bone turnover by virtue of the expression of their receptors on immature human osteoblast cell lines. PA and exercise have beneficial effects on health such as improving osteo-articular function, metabolic control, and QoL of people. Autonomic nervous system (ANS) and heart rate (HR) parameters can be used to analyse subjects' health and are also used to investigate stress and exercise level. Specifically, HR spectral analysis clarified the nature of diabetic autonomic neuropathy and other neurological disorders that favor ANS. Walking is a convenient low-impact mode of PA and is reported to be the most performed activity for those with diabetes. 10,000 steps/day are effective at improving glucose tolerance and lowering blood pressure in overweight, inactive women at risk for T2DM. Epidemiological studies have suggested that environmental factors and lifestyle changes may be responsible for the increased incidence of Thyroid Cancer (TC). Potential modifiable TC risk factors include insulin resistance and hyperinsulinemia. PA has an important impact on cholesterol, blood sugar, BMI and hba1c in the diabetic. Prolonged exercise has therapeutic effects. That is why, we chose to apply in our study, motor protocols for a period of 6 months (Fig. 3, 4, 5, 6). The American College of Sports Medicine and the American Diabetes Association have recommended at least 150 min/wk of moderate (50%-70% of an individual’s maximum heart rate) to vigorous (> 70% of an individual’s maximum heart rate) PA for patients with T2DM. The intensity of PA is assessed using the MET (metabolic equivalent) parameter. 1 MET is equal to the basal resting metabolic rate and an oxygen uptake of 3.5 mL/kg per minute. Controlled and adapted exercise in diabetes is a therapy, which could prevent the occurrence of complications associated with disease progression. The aging process leads to a degeneration of muscles, ligaments, bones and joints, but in the diabetic, you amplify and add vascular complications that can aggravate the problem. The WHO states that health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity. PA and physical exercise play a fundamental role in promoting positive lifestyle behaviours, capable of promoting health and wellness. It reduces the risk of developing diabetes and prevents important complications that can be fatal for the patient's life or in any case strongly disabling. Regular and moderate exercise improves the function of the immune system, reduces environmental and psychological stress, decreases the demand and administration of immunosuppressants. Moreover, it plays a decisive role in improving glucometabolic compensation and, in general, the subject's perception of his or her state of health, leading to a significant reduction in healthcare expenditure. A study conducted on QoL in diabetic patients, who were administered the two tests Sickness Impact Profile (SIP) and Functional Living Index (FLI), an index of psychosocial, physical and motor function, showed that QoL is not only related to the severity of the disease, treatment and complications, but also to subcultural elements, representing in fact a surprising parameter. As for our study, we had previously conducted searches in the scientific literature, which were in line with our research objective. Although the results produced highlighted the benefits of sport or PA in diabetes, on the other hand, we did not find any studies that considered the interaction of other behaviours (active vs. sedentary). Therefore, we set out to investigate the effects of an aerobic exercise programme in reducing BMI and blood glucose levels in obese subjects with T2DM, whether active or sedentary.
[Table: see text]