

Uric acid levels correlate with disease activity in growth hormone-secreting pituitary adenoma patients
- PMID: 37818085
- PMCID: PMC10561298
- DOI: 10.3389/fendo.2023.1230852
Uric acid levels correlate with disease activity in growth hormone-secreting pituitary adenoma patients
Abstract
Objective: Few studies reported the effects of growth hormone-secreting pituitary adenoma (GHPA) on uric acid (UA) metabolism and the relationship between growth hormone (GH)/insulin-like growth factor-1 (IGF-1) levels and UA are controversial. This study aimed to evaluate the relationship between IGF-1 and UA in patients with GHPA and to further clarify whether UA levels are associated with GHPA disease activity by follow-up.
Methods: A longitudinal study of 424 GHPA patients presenting to Beijing Tiantan Hospital, Capital Medical University between January 2015 and January 2023 was conducted. Spearman's correlation tests were performed to examine the relationship between IGF-1 and UA at baseline. Univariate and multivariate linear regression analysis was conducted to investigate the independent association between UA and IGF-1. Changes in postoperative IGF-1 and UA levels were followed prospectively, and the differences in UA levels between the biochemical remission and nonremission groups were compared.
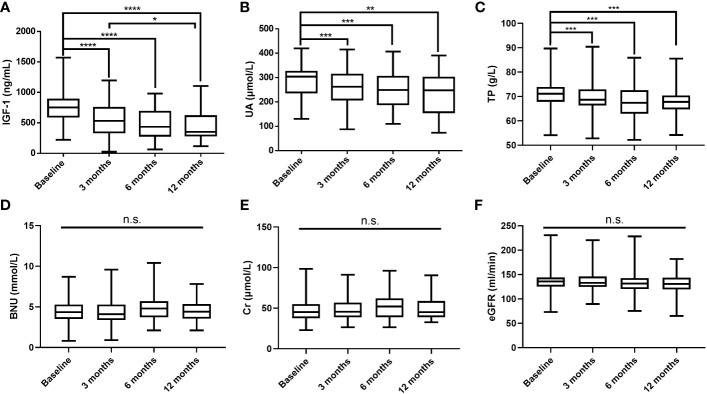
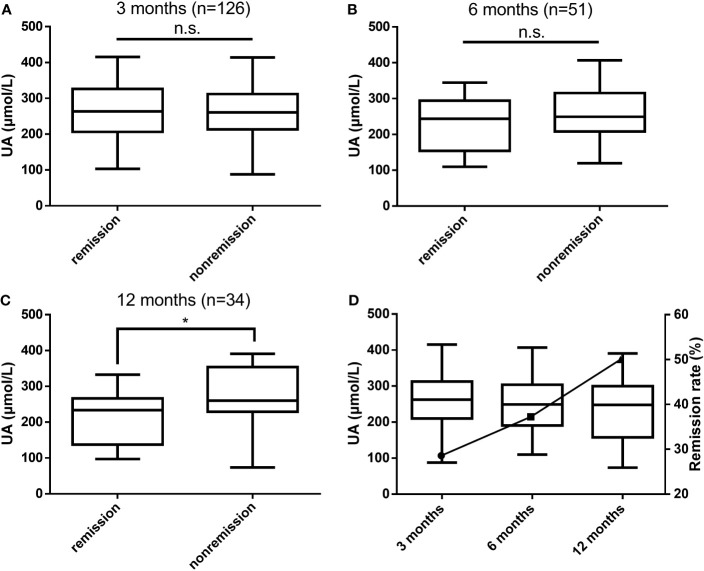
Results: At baseline, male patients, the lower the age, the higher the IGF-1 and body mass index (BMI), and the higher the UA levels. IGF-1 was significantly associated with UA after controlling for sex, age, and BMI (r = 0.122, P = 0.012). In adjusted multiple linear regression analysis, IGF-1 was independently associated with UA, and UA levels increased significantly with increasing IGF-1. During postoperative follow-up, UA decreased gradually as IGF-1 levels decreased. At 12 months postoperatively, UA levels were significantly lower in the biochemical remission group than in the nonremission group (P = 0.038).
Conclusions: In patients with GHPA, UA levels are associated with disease activity. Changes in UA levels should be taken into account in the comprehensive treatment of GHPA, patients presenting with HUA should be given lifestyle guidance and appropriate urate-lowering treatment according to their condition to better improve their prognosis.
Keywords: disease activity; growth hormone; growth hormone-secreting pituitary adenoma; insulin-like growth factor-1; uric acid.
Copyright © 2023 Mo, Chen, Wang, Guo, Wang, Tong and Zhong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Characteristics of Gut Microbiota in Patients with GH-Secreting Pituitary Adenoma.Microbiol Spectr. 2022 Feb 23;10(1):e0042521. doi: 10.1128/spectrum.00425-21. Epub 2022 Jan 12. Microbiol Spectr. 2022. PMID: 35019688 Free PMC article.
-
Growth hormone-secreting pituitary adenoma combined with Graves' disease: retrospective case series and literature review.Endocr Connect. 2024 Mar 4;13(4):e230439. doi: 10.1530/EC-23-0439. Print 2024 Apr 1. Endocr Connect. 2024. PMID: 38349236 Free PMC article.
-
Co-expression of multiple transcription factors is associated with clinical features and endocrine prognosis in growth hormone-secreting pituitary adenomas.Endocrine. 2025 Feb;87(2):788-799. doi: 10.1007/s12020-024-04082-x. Epub 2024 Oct 25. Endocrine. 2025. PMID: 39455511
-
Acromegaly.Pituitary. 2006;9(4):297-303. doi: 10.1007/s11102-006-0409-4. Pituitary. 2006. PMID: 17077948 Review.
-
Neuroendocrine tumors secreting growth hormone-releasing hormone: Pathophysiological and clinical aspects.Pituitary. 2006;9(3):221-9. doi: 10.1007/s11102-006-0267-0. Pituitary. 2006. PMID: 17036195 Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous