

Prospective comparison of prognostic scores for prediction of outcome after out-of-hospital cardiac arrest: results of the AfterROSC1 multicentric study
- PMID: 37819544
- PMCID: PMC10567621
- DOI: 10.1186/s13613-023-01195-w
Prospective comparison of prognostic scores for prediction of outcome after out-of-hospital cardiac arrest: results of the AfterROSC1 multicentric study
Abstract
Background: Out-of-hospital cardiac arrest (OHCA) is a heterogeneous entity with multiple origins and prognoses. An early, reliable assessment of the prognosis is useful to adapt therapeutic strategy, tailor intensity of care, and inform relatives. We aimed primarily to undertake a prospective multicentric study to evaluate predictive performance of the Cardiac Arrest Prognosis (CAHP) Score as compare to historical dataset systematically collected after OHCA (Utstein style criteria). Our secondary aim was to evaluate other dedicated scores for predicting outcome after OHCA and to compare them to Utstein style criteria.
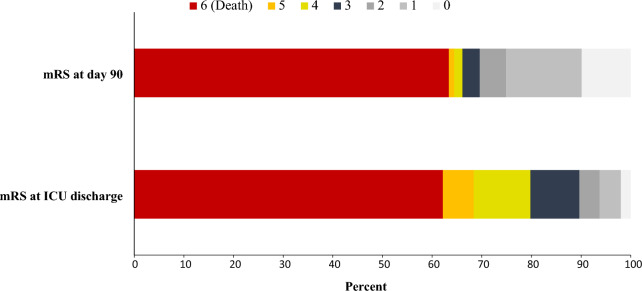
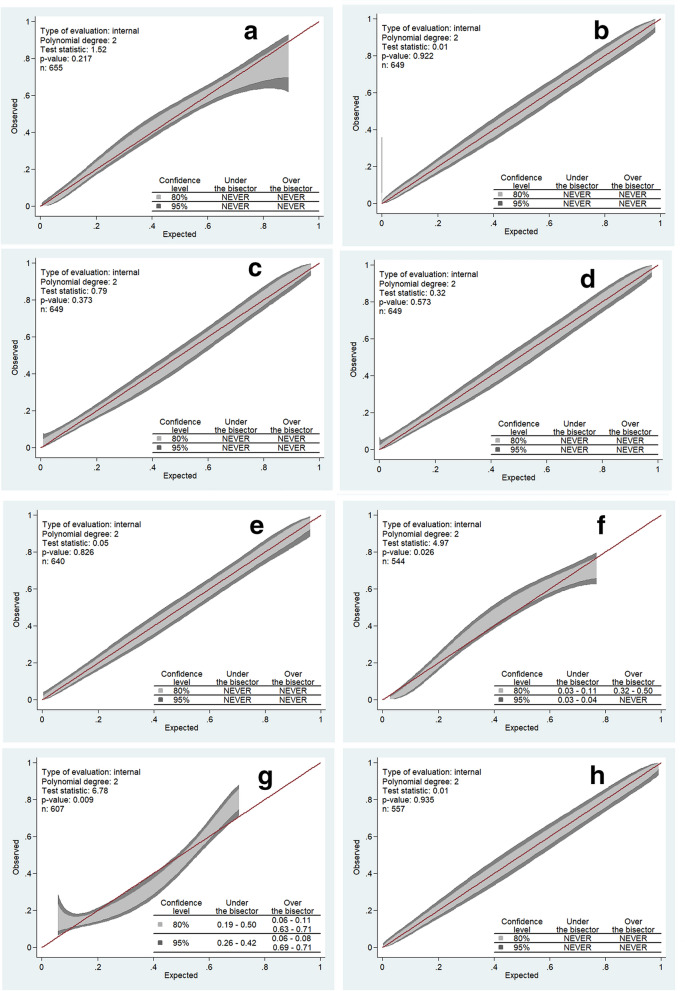
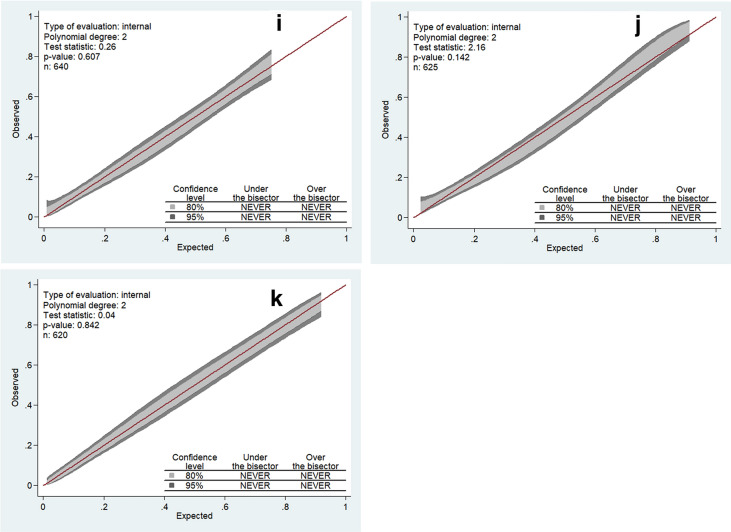
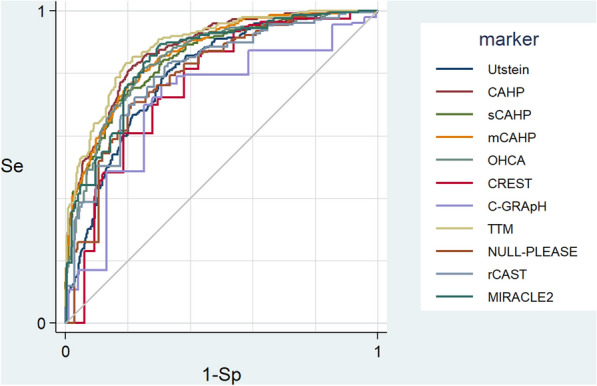
Methods: We prospectively collected data from 24 French and Belgium Intensive Care Units (ICUs) between August 2020 and June 2022. All cases of non-traumatic OHCA (cardiac and non-cardiac causes) patients with stable return of spontaneous circulation (ROSC) and comatose at ICU admission (defined by Glasgow coma score ≤ 8) on ICU admission were included. The primary outcome was the modified Rankin scale (mRS) at day 90 after cardiac arrest, assessed by phone interviews. A wide range of developed scores (CAHP, OHCA, CREST, C-Graph, TTM, CAST, NULL-PLEASE, and MIRACLE2) were included, and their accuracies in predicting poor outcome at 90 days after OHCA (defined as mRS ≥ 4) were determined using the area under the receiving operating characteristic curve (AUROC) and the calibration belt.
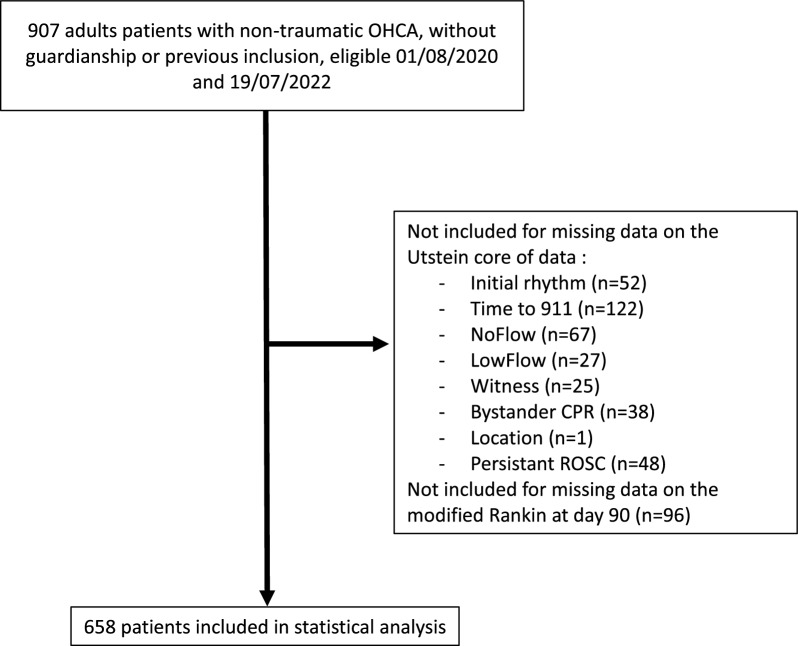
Results: During the study period, 907 patients were screened, and 658 were included in the study. Patients were predominantly male (72%), with a mean age of 61 ± 15, most having collapsed from a supposed cardiac cause (64%). The mortality rate at day 90 was 63% and unfavorable neurological outcomes were observed in 66%. The performance (AUROC) of Utstein criteria for poor outcome prediction was moderate at 0.79 [0.76-0.83], whereas AUROCs from other scores varied from 0.79 [0.75-0.83] to 0.88 [0.86-0.91]. For each score, the proportion of patients for whom individual values could not be calculated varied from 1.4% to 17.4%.
Conclusions: In patients admitted to ICUs after a successfully resuscitated OHCA, most of the scores available for the evaluation of the subsequent prognosis are more efficient than the usual Utstein criteria but calibration is unacceptable for some of them. Our results show that some scores (CAHP, sCAHP, mCAHP, OHCA, rCAST) have superior performance, and that their ease and speed of determination should encourage their use. Trial registration https://clinicaltrials.gov/ct2/show/NCT04167891.
Keywords: Cardiac arrest; Functional outcome; Neurological prognosis; Outcome prediction; Score.
© 2023. La Société de Réanimation de Langue Francaise = The French Society of Intensive Care (SRLF).
Conflict of interest statement
JBL received fees for lectures from BD and Zoll. GG received consulting fees from BD. AC received fees for lectures from BD. The other authors declare that they have no competing interests.
Figures
References
-
- Survival after out-of-hospital cardiac arrest in Europe - Results of the EuReCa TWO study - Resuscitation. https://www.resuscitationjournal.com/article/S0300-9572(20)30046-0/fulltext. Accessed 28 Sep 2021 - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
