

Survival Outcomes by Race and Ethnicity in Veterans With Nonmetastatic Castration-Resistant Prostate Cancer
- PMID: 37819658
- PMCID: PMC10568364
- DOI: 10.1001/jamanetworkopen.2023.37272
Survival Outcomes by Race and Ethnicity in Veterans With Nonmetastatic Castration-Resistant Prostate Cancer
Erratum in
-
Error in Byline.JAMA Netw Open. 2023 Nov 1;6(11):e2343869. doi: 10.1001/jamanetworkopen.2023.43869. JAMA Netw Open. 2023. PMID: 37910109 Free PMC article. No abstract available.
Abstract
Importance: Racial and ethnic disparities in prostate cancer are poorly understood. A given disparity-related factor may affect outcomes differently at each point along the highly variable trajectory of the disease.
Objective: To examine clinical outcomes by race and ethnicity in patients with nonmetastatic castration-resistant prostate cancer (nmCRPC) within the US Veterans Health Administration.
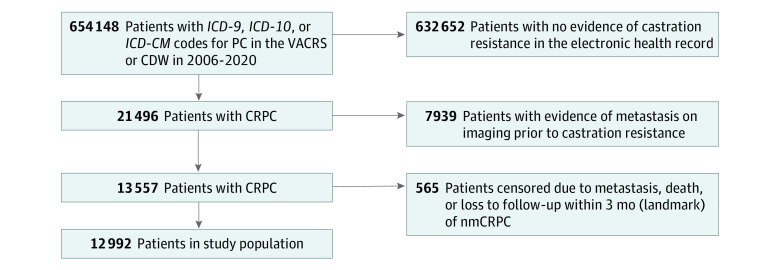
Design, setting, and participants: A retrospective, observational cohort study using electronic health care records (January 1, 2006, to December 31, 2021) in a nationwide equal-access health care system was conducted. Mean (SD) follow-up time was 4.3 (3.3) years. Patients included in the analysis were diagnosed with prostate cancer from January 1, 2006, to December 30, 2020, that progressed to nmCRPC defined by (1) increasing prostate-specific antigen levels, (2) ongoing androgen deprivation, and (3) no evidence of metastatic disease. Patients with metastatic disease or death within the landmark period (3 months after the first nmCRPC evidence) were excluded.
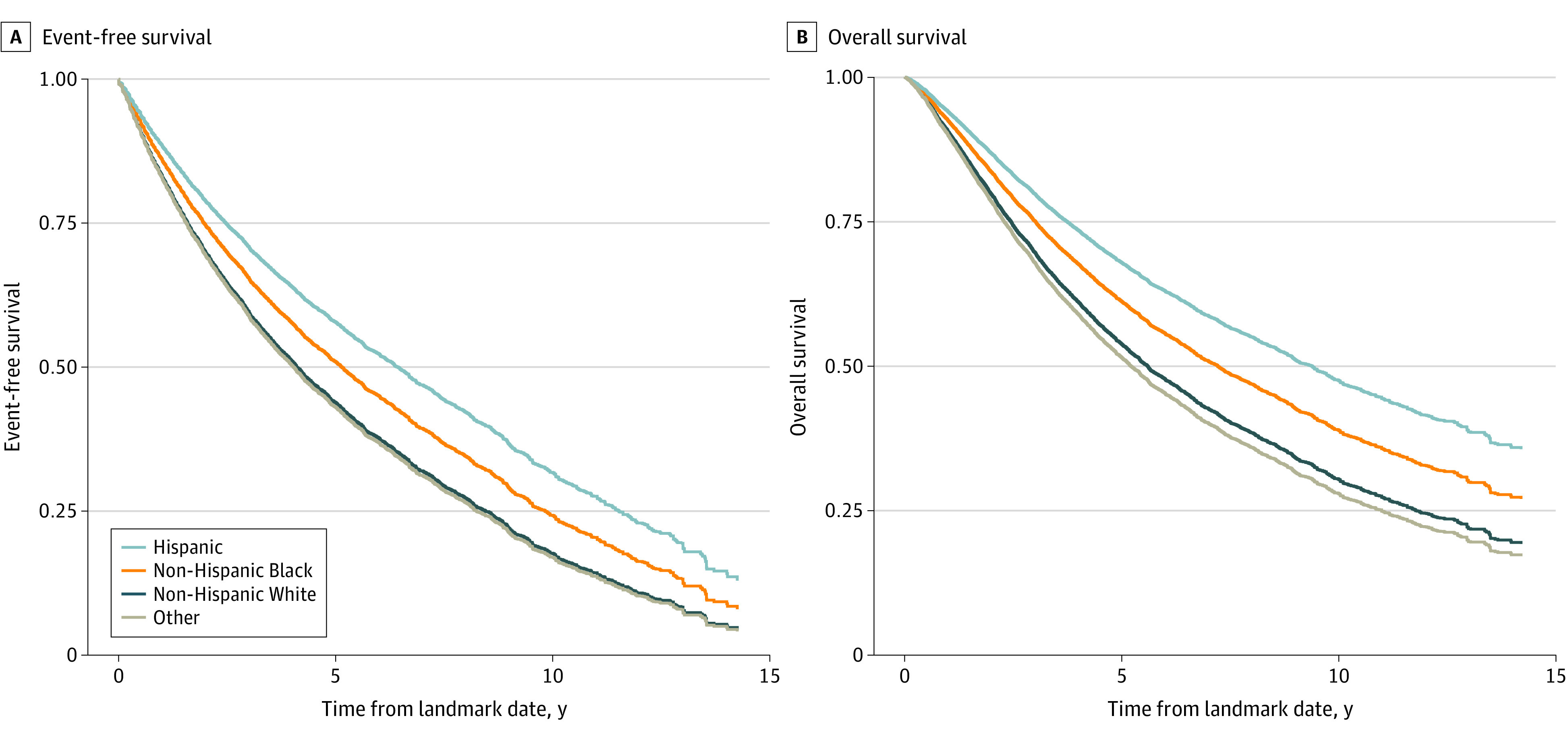
Main outcomes and measures: The primary outcome was time from the landmark period to death or metastasis; the secondary outcome was overall survival. A multivariate Cox proportional hazards model, Kaplan-Meier estimates, and adjusted survival curves were used to evaluate outcome differences by race and ethnicity.
Results: Of 12 992 patients in the cohort, 826 patients identified as Hispanic (6%), 3671 as non-Hispanic Black (28%; henceforth Black), 7323 as non-Hispanic White (56%; henceforth White), and 1172 of other race and ethnicity (9%; henceforth other, including American Indian or Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, unknown by patient, and patient declined to answer). Median time elapsed from nmCRPC to metastasis or death was 5.96 (95% CI, 5.58-6.34) years for Black patients, 5.62 (95% CI, 5.11-6.67) years for Hispanic patients, 4.11 (95% CI, 3.96-4.25) years for White patients, and 3.59 (95% CI, 3.23-3.97) years for other patients. Median unadjusted overall survival was 6.26 (95% CI, 6.03-6.46) years among all patients, 8.36 (95% CI, 8.0-8.8) years for Black patients, 8.56 (95% CI, 7.3-9.7) years for Hispanic patients, 5.48 (95% CI, 5.2-5.7) years for White patients, and 4.48 (95% CI, 4.1-5.0) years for other patients.
Conclusions and relevance: The findings of this cohort study of patients with nmCRPC suggest that differences in outcomes by race and ethnicity exist; in addition, Black and Hispanic men may have considerably improved outcomes when treated in an equal-access setting.
Conflict of interest statement
Figures
Similar articles
-
Racial and Ethnic Differences in Prostate Cancer Epidemiology Across Disease States in the VA.JAMA Netw Open. 2024 Nov 4;7(11):e2445505. doi: 10.1001/jamanetworkopen.2024.45505. JAMA Netw Open. 2024. PMID: 39546308 Free PMC article.
-
State Variation in Racial and Ethnic Disparities in Incidence of Triple-Negative Breast Cancer Among US Women.JAMA Oncol. 2023 May 1;9(5):700-704. doi: 10.1001/jamaoncol.2022.7835. JAMA Oncol. 2023. PMID: 36862439 Free PMC article.
-
Identifying and Mitigating Disparities in Central Line-Associated Bloodstream Infections in Minoritized Racial, Ethnic, and Language Groups.JAMA Pediatr. 2023 Jul 1;177(7):700-709. doi: 10.1001/jamapediatrics.2023.1379. JAMA Pediatr. 2023. PMID: 37252746 Free PMC article.
-
Race and Ethnicity Representation in Phase 2/3 Oncology Clinical Trial Publications: A Systematic Review.JAMA Health Forum. 2024 Jun 7;5(6):e241388. doi: 10.1001/jamahealthforum.2024.1388. JAMA Health Forum. 2024. PMID: 38848090 Free PMC article.
-
Racial/Ethnic Representation in United States and Australian Obstetric Research.Matern Child Health J. 2021 May;25(5):841-848. doi: 10.1007/s10995-020-03099-8. Epub 2020 Nov 22. Matern Child Health J. 2021. PMID: 33222026 Review.
Cited by
-
Real-world analyses of major adverse cardiovascular events and mortality risk after androgen deprivation therapy initiation in black vs. white prostate cancer patients.Prostate Cancer Prostatic Dis. 2025 Apr 18. doi: 10.1038/s41391-025-00963-y. Online ahead of print. Prostate Cancer Prostatic Dis. 2025. PMID: 40251347
-
Error in Byline.JAMA Netw Open. 2023 Nov 1;6(11):e2343869. doi: 10.1001/jamanetworkopen.2023.43869. JAMA Netw Open. 2023. PMID: 37910109 Free PMC article. No abstract available.
-
Development and validation of a machine learning-based risk model for metastatic disease in nmCRPC patients: a tumor marker prognostic study.Int J Surg. 2025 May 1;111(5):3331-3341. doi: 10.1097/JS9.0000000000002321. Int J Surg. 2025. PMID: 40143736 Free PMC article.
-
Androgen receptor pathway inhibitors and taxanes in metastatic prostate cancer: an outcome-adaptive randomized platform trial.Nat Med. 2024 Nov;30(11):3291-3302. doi: 10.1038/s41591-024-03204-2. Epub 2024 Aug 20. Nat Med. 2024. PMID: 39164518 Free PMC article. Clinical Trial.
-
Social Determinants of Health Mediate Racial Disparities in Cardiovascular Disease in Men With Prostate Cancer.JACC CardioOncol. 2024 Jun 18;6(3):390-401. doi: 10.1016/j.jaccao.2024.04.004. eCollection 2024 Jun. JACC CardioOncol. 2024. PMID: 38983382 Free PMC article.
References
-
- Smedley BD, Stith AY, Nelson AR, eds; Institute of Medicine (US) Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care . Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. National Academies Press; 2003. - PubMed
-
- Butler M, McCreedy E, Schwer N, et al. . Improving Cultural Competence to Reduce Health Disparities. Agency for Healthcare Research and Quality; 2016. - PubMed
