

Adjunctive Dexamethasone for Tuberculous Meningitis in HIV-Positive Adults
- PMID: 37819954
- PMCID: PMC7615197
- DOI: 10.1056/NEJMoa2216218
Adjunctive Dexamethasone for Tuberculous Meningitis in HIV-Positive Adults
Abstract
Background: Adjunctive glucocorticoids are widely used to treat human immunodeficiency virus (HIV)-associated tuberculous meningitis despite limited data supporting their safety and efficacy.
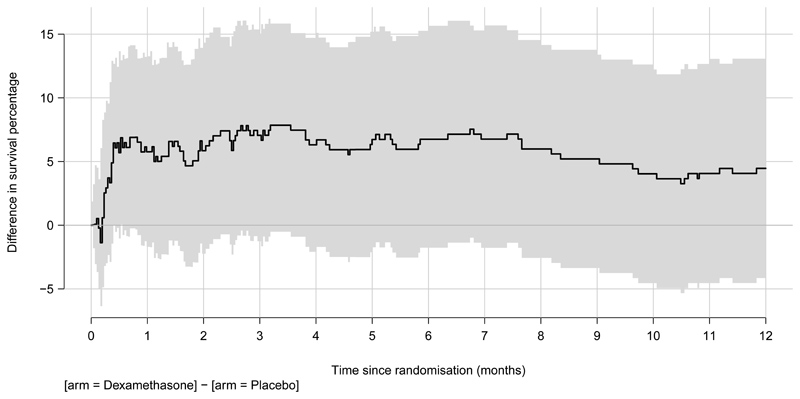
Methods: We conducted a double-blind, randomized, placebo-controlled trial involving HIV-positive adults (≥18 years of age) with tuberculous meningitis in Vietnam and Indonesia. Participants were randomly assigned to receive a 6-to-8-week tapering course of either dexamethasone or placebo in addition to 12 months of antituberculosis chemotherapy. The primary end point was death from any cause during the 12 months after randomization.
Results: A total of 520 adults were randomly assigned to receive either dexamethasone (263 participants) or placebo (257 participants). The median age was 36 years; 255 of 520 participants (49.0%) had never received antiretroviral therapy, and 251 of 484 participants (51.9%) with available data had a baseline CD4 count of 50 cells per cubic millimeter or less. Six participants withdrew from the trial, and five were lost to follow-up. During the 12 months of follow-up, death occurred in 116 of 263 participants (44.1%) in the dexamethasone group and in 126 of 257 participants (49.0%) in the placebo group (hazard ratio, 0.85; 95% confidence interval, 0.66 to 1.10; P = 0.22). Prespecified analyses did not reveal a subgroup that clearly benefited from dexamethasone. The incidence of secondary end-point events, including cases of immune reconstitution inflammatory syndrome during the first 6 months, was similar in the two trial groups. The numbers of participants with at least one serious adverse event were similar in the dexamethasone group (192 of 263 participants [73.0%]) and the placebo group (194 of 257 participants [75.5%]) (P = 0.52).
Conclusions: Among HIV-positive adults with tuberculous meningitis, adjunctive dexamethasone, as compared with placebo, did not confer a benefit with respect to survival or any secondary end point. (Funded by the Wellcome Trust; ACT HIV ClinicalTrials.gov number, NCT03092817.).
Copyright © 2023 Massachusetts Medical Society.
Figures


Comment in
-
Dexamethasone for Tuberculous Meningitis in HIV-Positive Adults.N Engl J Med. 2024 Jan 25;390(4):382-383. doi: 10.1056/NEJMc2313671. N Engl J Med. 2024. PMID: 38265655 No abstract available.
-
Dexamethasone for Tuberculous Meningitis in HIV-Positive Adults. Reply.N Engl J Med. 2024 Jan 25;390(4):383. doi: 10.1056/NEJMc2313671. N Engl J Med. 2024. PMID: 38265656 No abstract available.
References
-
- Thwaites GE, Bang ND, Dung NH, et al. Dexamethasone for the Treatment of Tuberculous Meningitis in Adolescents and Adults. N Engl J Med. 2004;351:1741–51. - PubMed
-
- Ruslami R, Ganiem AR, Dian S, et al. Intensified regimen containing rifampicin and moxifloxacin for tuberculous meningitis: an open-label, randomised controlled phase 2 trial. Lancet Infect Dis. 2013;13:27–35. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials